You might also like
- TOR-Senior Consultant-Infrastructure (NHM, MoH&FW)Document2 pagesTOR-Senior Consultant-Infrastructure (NHM, MoH&FW)ashish kumarNo ratings yet
- SBI PO Notification 2019Document4 pagesSBI PO Notification 2019learning duniaNo ratings yet
- VMD-422 Questions - (II)Document8 pagesVMD-422 Questions - (II)ਰੋਹਿਤ ਬਾਵਾNo ratings yet
- Oscar + GK ListDocument25 pagesOscar + GK Listashish kumarNo ratings yet
- TNPSC VAS Preparatory Guide Part IIDocument58 pagesTNPSC VAS Preparatory Guide Part IIVinoth VinoNo ratings yet
- Interview Result Cutoff Marks RPSC JR Legal Officer Posts Reserve ListDocument2 pagesInterview Result Cutoff Marks RPSC JR Legal Officer Posts Reserve Listashish kumarNo ratings yet
- VMD-421 (1st Sept 2014)Document13 pagesVMD-421 (1st Sept 2014)Santosh BhandariNo ratings yet
- "Indo-Tibetan Border Police Force": (Ministry of Home Affairs) Govt. of IndiaDocument20 pages"Indo-Tibetan Border Police Force": (Ministry of Home Affairs) Govt. of Indiaakash nairNo ratings yet
- VMD-412 9 April 2014Document8 pagesVMD-412 9 April 2014ashish kumarNo ratings yet
- VMD-411 2 April 2014Document10 pagesVMD-411 2 April 2014Kadapavets kadapavasNo ratings yet
- VMD-411 2 April 2014Document10 pagesVMD-411 2 April 2014Kadapavets kadapavasNo ratings yet
- Arawali Veterinary College Bajor, SikarDocument8 pagesArawali Veterinary College Bajor, Sikarashish kumarNo ratings yet
- Test 2Document1 pageTest 2ashish kumarNo ratings yet
- Unit Test-4Document7 pagesUnit Test-4ashish kumarNo ratings yet
- Unit Test-5Document4 pagesUnit Test-5ashish kumarNo ratings yet
- Unit Test-6Document6 pagesUnit Test-6ashish kumarNo ratings yet
- IDBI Assistant Manager Recruitment 2019.PDF-92Document20 pagesIDBI Assistant Manager Recruitment 2019.PDF-92Subham GhoshNo ratings yet
- Notification IDBI Bank Executive PostsDocument22 pagesNotification IDBI Bank Executive Postsashish kumarNo ratings yet
- Suturetrainingcourse 140320061235 Phpapp01Document50 pagesSuturetrainingcourse 140320061235 Phpapp01hazeemmegahedNo ratings yet
- Advance Techniques in Traumatic Reticuloperitonitis Diagnosis: ReviewDocument8 pagesAdvance Techniques in Traumatic Reticuloperitonitis Diagnosis: Reviewashish kumarNo ratings yet
- Diseases of NeonatesDocument8 pagesDiseases of Neonatesashish kumarNo ratings yet
- Notification IDBI Bank Executive PostsDocument22 pagesNotification IDBI Bank Executive Postsashish kumarNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- XDM-100 IOM SDH A00 4-5 enDocument334 pagesXDM-100 IOM SDH A00 4-5 endilipgulatiNo ratings yet
- "Assessing The Effect of Work Overload On Employees Job Satisfaction" Case of Commercial Bank of Ethiopia Nekemte Town BranchesDocument1 page"Assessing The Effect of Work Overload On Employees Job Satisfaction" Case of Commercial Bank of Ethiopia Nekemte Town Branchesmikiyas zerihunNo ratings yet
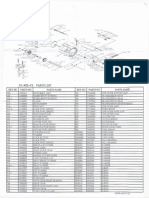
- Okuma CL302L Parts List & ManualDocument3 pagesOkuma CL302L Parts List & Manualcoolestkiwi100% (1)
- H2S Personal Gas MonitorDocument14 pagesH2S Personal Gas Monitormaher mansiNo ratings yet
- Diversity of Tree Vegetation of Rajasthan, India: Tropical Ecology September 2014Document9 pagesDiversity of Tree Vegetation of Rajasthan, India: Tropical Ecology September 2014Abdul WajidNo ratings yet
- Indiga Indiga: Tech TechDocument32 pagesIndiga Indiga: Tech Techsunny100% (1)
- Rubricks For Case StudyDocument2 pagesRubricks For Case StudyMiguelito Aquino RuelanNo ratings yet
- 05 N141 31673Document21 pages05 N141 31673priya thakurNo ratings yet
- Beyond Investment: The Power of Capacity-Building SupportDocument44 pagesBeyond Investment: The Power of Capacity-Building SupportLaxNo ratings yet
- 3.3 Motherboard SchematicsDocument49 pages3.3 Motherboard SchematicsJoanna WęgielNo ratings yet
- Past:: Simple Indefinite Continuous Perfect Perfect ContinuousDocument12 pagesPast:: Simple Indefinite Continuous Perfect Perfect ContinuousAhmed Abd El HafeezNo ratings yet
- Huawei Sne Mobile Phone User Guide - (Emui9.0.1 - 01, En-Uk, Normal)Document68 pagesHuawei Sne Mobile Phone User Guide - (Emui9.0.1 - 01, En-Uk, Normal)FarzadNo ratings yet
- Aims and Principles of Foreign Language TeachingDocument3 pagesAims and Principles of Foreign Language TeachingresearchparksNo ratings yet
- Instagram Marketing PDFDocument72 pagesInstagram Marketing PDFneeloufershaik100% (1)
- Sonos Outdoor by Sonance Installation ManualDocument4 pagesSonos Outdoor by Sonance Installation Manualvlad111No ratings yet
- Benjamin Gomez v. Enrico PalomarDocument11 pagesBenjamin Gomez v. Enrico PalomarUlyung DiamanteNo ratings yet
- Value For Money Analysis.5.10.12Document60 pagesValue For Money Analysis.5.10.12Jason SanchezNo ratings yet
- COT RPMS Rating Sheet For T I III For SY 2021 2022 JhanzDocument2 pagesCOT RPMS Rating Sheet For T I III For SY 2021 2022 Jhanzjhancelle golosindaNo ratings yet
- NDC Format For Billing PADDocument3 pagesNDC Format For Billing PADShantkumar ShingnalliNo ratings yet
- Executive MBA Project - Self Help Allowance - FinalDocument55 pagesExecutive MBA Project - Self Help Allowance - FinalKumar SourabhNo ratings yet
- Advance Strategic Marketing: Project Report of Nayatel.Document46 pagesAdvance Strategic Marketing: Project Report of Nayatel.Omer Abbasi60% (15)
- Leadership's Ramdom MCQsDocument48 pagesLeadership's Ramdom MCQsAhmed NoumanNo ratings yet
- Jimerson Rampola Final DemoDocument64 pagesJimerson Rampola Final DemoJIMERSON RAMPOLANo ratings yet
- Analyzing Your Data and Drawing Conclusions Worksheet Without AnswersDocument3 pagesAnalyzing Your Data and Drawing Conclusions Worksheet Without AnswersNur ShaNo ratings yet
- INST240 Sec4Document127 pagesINST240 Sec4bhanu6212No ratings yet
- Voting BehaviorDocument23 pagesVoting BehaviorWela Paing FallitangNo ratings yet
- Distress Manual PDFDocument51 pagesDistress Manual PDFEIRINI ZIGKIRIADOUNo ratings yet
- H-Beam Catalogue JindalDocument4 pagesH-Beam Catalogue JindalVikram DalalNo ratings yet
- Aviation EbookDocument36 pagesAviation Ebookmeroka2000No ratings yet
- Automatic Link EstablishmentDocument7 pagesAutomatic Link EstablishmenthaikalNo ratings yet