You might also like
- It's Not Just a Heavy Period; The Miscarriage HandbookFrom EverandIt's Not Just a Heavy Period; The Miscarriage HandbookRating: 2 out of 5 stars2/5 (1)
- Ectopic Pregnancy: Medlineplus TopicsDocument9 pagesEctopic Pregnancy: Medlineplus TopicsJonathan BendecioNo ratings yet
- Questions in CasesDocument10 pagesQuestions in CasesRoselyn VelascoNo ratings yet
- Brief DescriptionDocument7 pagesBrief DescriptionPrincess Pilove GawongnaNo ratings yet
- Gestational Conditions 1Document19 pagesGestational Conditions 1MrLarry Dolor100% (1)
- Classification: Miscarriage or Spontaneous Abortion Is The Spontaneous End of A Pregnancy at ADocument9 pagesClassification: Miscarriage or Spontaneous Abortion Is The Spontaneous End of A Pregnancy at AAnn GelaNo ratings yet
- Midwifery 102 Module 1Document10 pagesMidwifery 102 Module 1WynJoy NebresNo ratings yet
- Miscarriage What Is It?Document4 pagesMiscarriage What Is It?Suseno AjiNo ratings yet
- Bleeding During PregnancyDocument69 pagesBleeding During PregnancyMohnnad Hmood AlgaraybhNo ratings yet
- Ectopic Pregnancy: Causes, Symptoms & TreatmentDocument10 pagesEctopic Pregnancy: Causes, Symptoms & TreatmentXo Yem0% (1)
- Threatened Abortion PDFDocument3 pagesThreatened Abortion PDFAizat KamalNo ratings yet
- Ectopic PregnancyDocument26 pagesEctopic PregnancyMalek.Fakher1900No ratings yet
- NCM 109 - Care of Mother, Child at Risk or With Problems: St. Paul University Philippines Tuguegarao City, Cagayan 3500Document6 pagesNCM 109 - Care of Mother, Child at Risk or With Problems: St. Paul University Philippines Tuguegarao City, Cagayan 3500Kristiene Kyle Aquino0% (1)
- Abortionsource 100605123737 Phpapp01Document38 pagesAbortionsource 100605123737 Phpapp01Erina Erichan OtoNo ratings yet
- Ectopic PregnancyDocument5 pagesEctopic PregnancyFaith FuentevillaNo ratings yet
- Uterus: Signs and SymptomsDocument11 pagesUterus: Signs and SymptomsJoy Parallag - BautoNo ratings yet
- Causes, Symptoms and Treatment of Hydatidiform MoleDocument15 pagesCauses, Symptoms and Treatment of Hydatidiform MoleRegine Mae Morales EncinadaNo ratings yet
- Complications During Pregnancy - Chapt 5Document93 pagesComplications During Pregnancy - Chapt 5klyde_evangelistaNo ratings yet
- Ectopic Pregnancy - OMDocument9 pagesEctopic Pregnancy - OMrheindNo ratings yet
- Case Study MiscariageDocument14 pagesCase Study MiscariagesexiiimammaNo ratings yet
- Incomplete AbortionDocument4 pagesIncomplete AbortionAira Jane MuñozNo ratings yet
- Case Study Presentation: "Ectopic Pregnancy"Document8 pagesCase Study Presentation: "Ectopic Pregnancy"Sherwina Alih-BieberNo ratings yet
- Ectopic Pregnancy GuideDocument15 pagesEctopic Pregnancy GuideVanessa Santos100% (1)
- INTRODUCTIO1Document10 pagesINTRODUCTIO1Diane ChuNo ratings yet
- Ass Ectopic PregnancyDocument10 pagesAss Ectopic PregnancyPriyaNo ratings yet
- Factors Increasing Risk of Female Reproductive DisordersDocument6 pagesFactors Increasing Risk of Female Reproductive DisordersjoannaNo ratings yet
- Case Study - Incomplete Abortion Related To APSDocument8 pagesCase Study - Incomplete Abortion Related To APSRomeo ReyesNo ratings yet
- Elizabeth G. Querubin BSN 3E1-9 - Group 195 A Ectopic PregnancyDocument16 pagesElizabeth G. Querubin BSN 3E1-9 - Group 195 A Ectopic PregnancyLizeth Querubin97% (38)
- Early Pregnancy Loss - Practice Essentials, Background, PathophysiologyDocument10 pagesEarly Pregnancy Loss - Practice Essentials, Background, PathophysiologyAldair SanchezNo ratings yet
- Hyperemesis GravidarumDocument6 pagesHyperemesis GravidarumMary Ann YumulNo ratings yet
- NCM 109-Module 1 Lesson 2Document31 pagesNCM 109-Module 1 Lesson 2MARY ROSE DOLOGUINNo ratings yet
- Early Pregnancy Bleeding Causes and TypesDocument51 pagesEarly Pregnancy Bleeding Causes and TypesMesk Banat100% (2)
- Submitted By: Diana M. Resultay A301/Group-3B Submitted To: Ms. ReyesDocument9 pagesSubmitted By: Diana M. Resultay A301/Group-3B Submitted To: Ms. ReyesDiannetotz MoralesNo ratings yet
- Postpartum Clinical QuizDocument6 pagesPostpartum Clinical QuizAmy100% (1)
- NCM 109 Module 1 Lesson 2Document31 pagesNCM 109 Module 1 Lesson 2shekinahhuzsumangilNo ratings yet
- Uterus: Signs and SymptomsDocument4 pagesUterus: Signs and SymptomsmoigomezNo ratings yet
- Uterus: Signs and SymptomsDocument4 pagesUterus: Signs and SymptomsmoigomezNo ratings yet
- Ectopic Pregnancy: Causes, Symptoms, Diagnosis and TreatmentDocument15 pagesEctopic Pregnancy: Causes, Symptoms, Diagnosis and TreatmentPrincess Huey GreyNo ratings yet
- Presentation 1Document53 pagesPresentation 1Nor Ubudiah SetiNo ratings yet
- Ectopic Pregnancy Kehamilan Luar RahimDocument5 pagesEctopic Pregnancy Kehamilan Luar RahimMuhamad Aminuddin Abu BakarNo ratings yet
- StillbirthDocument4 pagesStillbirthTubagus Siswadi WijaksanaNo ratings yet
- Complication of Pregnancy Uterine Cavity: 1 Classification 1.1 Tubal Pregnancy 1.2 Nontubal Ectopic PregnancyDocument41 pagesComplication of Pregnancy Uterine Cavity: 1 Classification 1.1 Tubal Pregnancy 1.2 Nontubal Ectopic Pregnancyゴンサレス マリオ ジョンNo ratings yet
- Hyperemesis Gravidarum: By: Solomon Berhe OBGYN ResidentDocument73 pagesHyperemesis Gravidarum: By: Solomon Berhe OBGYN Residentmuleget haileNo ratings yet
- Threatened Abortion ReportDocument8 pagesThreatened Abortion ReportMohamad RaisNo ratings yet
- MiscariageDocument17 pagesMiscariagemitchillNo ratings yet
- 9 Antepartum CareDocument24 pages9 Antepartum CareFlowerer ShafaaNo ratings yet
- High - Risk PregnancyDocument110 pagesHigh - Risk PregnancyAndre DityaNo ratings yet
- AbortionDocument19 pagesAbortionAhmed SabryNo ratings yet
- Vaginal Bleeding in Early PregnancyDocument8 pagesVaginal Bleeding in Early PregnancyBal Ri Mekoleu100% (1)
- Case Study #1: AbortionDocument42 pagesCase Study #1: AbortionJhoanne DelloroNo ratings yet
- Ectopic PregnancyDocument17 pagesEctopic PregnancyB.HemavarshiniNo ratings yet
- NCM 109-Module 1 Lesson 1Document30 pagesNCM 109-Module 1 Lesson 1MARY ROSE DOLOGUINNo ratings yet
- Rejina Raita Class - Xii Roll No-Mr. Ashutosh Subudhi: Abortion in IndiaDocument12 pagesRejina Raita Class - Xii Roll No-Mr. Ashutosh Subudhi: Abortion in IndiaCSC LanjipadarNo ratings yet
- Acog Nausea Vomiting PregnancyDocument13 pagesAcog Nausea Vomiting PregnancymispNo ratings yet
- Prenatal care guideDocument31 pagesPrenatal care guideNoraNo ratings yet
- Are You Fertile?: Guides on Healthy Lifestyles that Increases Fertility Chances in Men and WomenFrom EverandAre You Fertile?: Guides on Healthy Lifestyles that Increases Fertility Chances in Men and WomenNo ratings yet
- Conceive A Baby Naturally - How To Cure Infertility And Get Pregnant NaturallyFrom EverandConceive A Baby Naturally - How To Cure Infertility And Get Pregnant NaturallyNo ratings yet
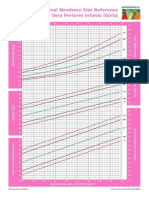
- Intergrowth21 Newborn Size Reference Charts (Girls)Document2 pagesIntergrowth21 Newborn Size Reference Charts (Girls)Anonymous MWd5UOUuiyNo ratings yet
- ALSO ManualDocument466 pagesALSO Manualemkay1234No ratings yet
- mrmbs ppt (1) (1)Document7 pagesmrmbs ppt (1) (1)ASHNo ratings yet
- Obstetrics QuestionsDocument22 pagesObstetrics QuestionsShaik AmreenNo ratings yet
- StillbirthDocument4 pagesStillbirthTubagus Siswadi WijaksanaNo ratings yet
- Management of PPHDocument1 pageManagement of PPH098 U.KARTHIK SARAVANA KANTHNo ratings yet
- Multifetal Pregnancy: Dr. Hani MahdiDocument59 pagesMultifetal Pregnancy: Dr. Hani MahdiArwa QishtaNo ratings yet
- All India Institute of Medical Sciences, Jodhpur College of Nursing Lesson Plan ON TopicDocument12 pagesAll India Institute of Medical Sciences, Jodhpur College of Nursing Lesson Plan ON TopicFarheen khanNo ratings yet
- Workshop In-Alarm: Scientific Program Pre - CongressDocument3 pagesWorkshop In-Alarm: Scientific Program Pre - Congressdaniel_alexander_susenoNo ratings yet
- Equipment Tray For Postpartum Hemorrhage: T. F. BaskettDocument4 pagesEquipment Tray For Postpartum Hemorrhage: T. F. BaskettsalijanstarNo ratings yet
- Emergency Obstetric Care in The Prevention of Maternal MortalityDocument9 pagesEmergency Obstetric Care in The Prevention of Maternal Mortalityapi-3705046No ratings yet
- 2020 Article 2890 PDFDocument8 pages2020 Article 2890 PDFyenny handayani sihiteNo ratings yet
- Dapus DsDocument3 pagesDapus DsLailatul MasrurohNo ratings yet
- Antepartum Haemorrage (APH) : Dr. Mtumweni, MDDocument42 pagesAntepartum Haemorrage (APH) : Dr. Mtumweni, MDmarco luenaNo ratings yet
- Obstetric Violence - A Latin American Legal Response To Mistreatment During ChildbirthDocument4 pagesObstetric Violence - A Latin American Legal Response To Mistreatment During ChildbirthAnaNo ratings yet
- High RiskDocument38 pagesHigh RiskDiana Rose R. Ulep100% (1)
- Daftar Pustaka ObgynDocument1 pageDaftar Pustaka ObgynISMJNo ratings yet
- Case Presentation Placenta PreviaDocument37 pagesCase Presentation Placenta PreviaJasmin Sabna100% (2)
- Early Pregnancy Bleeding Causes and TypesDocument51 pagesEarly Pregnancy Bleeding Causes and TypesMesk Banat100% (2)
- Meconium PpromDocument7 pagesMeconium Ppromkutra3000No ratings yet
- النسا في رغيف Breif fe Re3eefDocument46 pagesالنسا في رغيف Breif fe Re3eefWael HamdyNo ratings yet
- Obstetrics: Antenatal Care IncludesDocument11 pagesObstetrics: Antenatal Care Includesapi-3829364No ratings yet
- Leopold's Maneuver JournalDocument5 pagesLeopold's Maneuver JournalGeevine CansinoNo ratings yet
- ABORTIONDocument23 pagesABORTIONCristyl Shine BariaoNo ratings yet
- Obstetrics and Gynecology WordsDocument1 pageObstetrics and Gynecology WordsDiah Wardana0% (1)
- Obs 7th Sem Mid TermDocument5 pagesObs 7th Sem Mid Termaparna shama100% (1)
- Society For Maternal-Fetal Medicine Consult Series #52: Diagnosis and Management of Fetal Growth RestrictionDocument16 pagesSociety For Maternal-Fetal Medicine Consult Series #52: Diagnosis and Management of Fetal Growth RestrictionRaul DoctoNo ratings yet
- R1 Symptoms and Diagnosis of PregnancyDocument49 pagesR1 Symptoms and Diagnosis of PregnancyMoges desaleNo ratings yet
- California Prenatal Screening HandbookDocument48 pagesCalifornia Prenatal Screening Handbookrolla_hiraNo ratings yet
- Quantitative Blood Loss in Obstetric Hemorrhage .40Document7 pagesQuantitative Blood Loss in Obstetric Hemorrhage .40Santiago MoraNo ratings yet