You might also like
- Health informatics: Improving patient careFrom EverandHealth informatics: Improving patient careBCS, The Chartered Institute for ITRating: 3 out of 5 stars3/5 (1)
- Qualified Confidentiality, Patient Safety and Freedom of InformationDocument6 pagesQualified Confidentiality, Patient Safety and Freedom of InformationpatientsafetyNo ratings yet
- Towards Consensus For Best Practice: Use of Patient Records From General Practice For ResearchDocument37 pagesTowards Consensus For Best Practice: Use of Patient Records From General Practice For ResearchWellcome TrustNo ratings yet
- Abouelmehdi2018 Article BigHealthcareDataPreservingSecDocument18 pagesAbouelmehdi2018 Article BigHealthcareDataPreservingSecorionUPCNo ratings yet
- Study Health Care ReportDocument54 pagesStudy Health Care ReportJawad ShahNo ratings yet
- Confidentiality: NHS Code of PracticeDocument52 pagesConfidentiality: NHS Code of PracticeGeorge J. CooganNo ratings yet
- Patient Safety in RadoncDocument4 pagesPatient Safety in Radoncapi-575843507No ratings yet
- Roils PaperDocument4 pagesRoils Paperapi-575843507No ratings yet
- Book ChapterDocument6 pagesBook Chapterabdul adilNo ratings yet
- nigeriaDocument10 pagesnigeriamohamedNo ratings yet
- Rough 2Document7 pagesRough 2johnessamburuNo ratings yet
- Therapeutic Communication: (Document Subtitle)Document9 pagesTherapeutic Communication: (Document Subtitle)High TechNo ratings yet
- Arti Ficial Intelligence-Based Clinical Decision Support in Modern Medical Physics: Selection, Acceptance, Commissioning, and Quality AssuranceDocument8 pagesArti Ficial Intelligence-Based Clinical Decision Support in Modern Medical Physics: Selection, Acceptance, Commissioning, and Quality AssuranceDhanalakshmi PNo ratings yet
- Radiation Safety PaperDocument4 pagesRadiation Safety Paperapi-632529930No ratings yet
- Thesis on DiagnosticsDocument2 pagesThesis on Diagnosticsharshini kishore singhNo ratings yet
- Hassling2003 Article AWeb-BasedPatientInformationSyDocument12 pagesHassling2003 Article AWeb-BasedPatientInformationSyddineshkumar51144No ratings yet
- 2007 - Privacy and Confidentiality of Health Information - Ndian Journal of Medical EthicsDocument1 page2007 - Privacy and Confidentiality of Health Information - Ndian Journal of Medical EthicsDr. Rajesh Kumar SinhaNo ratings yet
- ASSIGNMENTDocument8 pagesASSIGNMENTPharmanic By Ruttaba FatimaNo ratings yet
- Storage Standards and Solutions Data Storage ShariDocument36 pagesStorage Standards and Solutions Data Storage Sharijmarcos.whoscallNo ratings yet
- Ijerph 20 07112Document17 pagesIjerph 20 07112Hina SardarNo ratings yet
- Big Data Security in Healthcare 1Document8 pagesBig Data Security in Healthcare 1International Journal of Innovative Science and Research TechnologyNo ratings yet
- Monitoring Preventable Adverse Events and Near.9Document6 pagesMonitoring Preventable Adverse Events and Near.9danny widjajaNo ratings yet
- Envisioning A Learning Healthcare SystemDocument6 pagesEnvisioning A Learning Healthcare SystemOmWawanNo ratings yet
- NSQHS Standards Fact Sheet Standard 6Document2 pagesNSQHS Standards Fact Sheet Standard 6Annette LowryNo ratings yet
- Tele MedicineDocument12 pagesTele MedicineNoorul Faedzah RosliNo ratings yet
- Mckane Radsafety PaperDocument4 pagesMckane Radsafety Paperapi-569589889No ratings yet
- Yorkshire Centre For Health InformaticsDocument18 pagesYorkshire Centre For Health InformaticsMark HawkerNo ratings yet
- Narrative Medicine: Feasibility of A Digital Narrative Diary Application in OncologyDocument12 pagesNarrative Medicine: Feasibility of A Digital Narrative Diary Application in OncologyTeuku FadhliNo ratings yet
- J Evidence Based Medicine - 2020 - Yang - Brief Introduction of Medical Database and Data Mining Technology in Big Data EraDocument13 pagesJ Evidence Based Medicine - 2020 - Yang - Brief Introduction of Medical Database and Data Mining Technology in Big Data EraMartha Isabel BurgosNo ratings yet
- Big DataDocument3 pagesBig Datamaestria20090No ratings yet
- Jurnal Telenursing Athiqah Syukri 2BDocument2 pagesJurnal Telenursing Athiqah Syukri 2BAthiqah SyukriNo ratings yet
- An Agile Approach To Accelerate Development and Adoption of Electronic Product Information StandardsDocument23 pagesAn Agile Approach To Accelerate Development and Adoption of Electronic Product Information StandardschronakiNo ratings yet
- Using ICT in SchoolDocument5 pagesUsing ICT in Schoolsiti syuhada binti zainalNo ratings yet
- Governance of AI in HealthcareDocument9 pagesGovernance of AI in Healthcareyulita basirNo ratings yet
- Brief Introduction of Medical Database and Data MiDocument13 pagesBrief Introduction of Medical Database and Data MiXenia RepuelaNo ratings yet
- New Project CombinedDocument10 pagesNew Project CombinedMorondiya Oluwadamilare OluwatimilehinNo ratings yet
- Practical Approaches To Creating A Security CultureDocument7 pagesPractical Approaches To Creating A Security CultureEPNo ratings yet
- Epf Ai in HealthcareDocument11 pagesEpf Ai in Healthcarewaludde conradNo ratings yet
- Perceptions and Experiences of Childhood Vaccination Communication Strategies Among Caregivers and Health Workers in Nigeria: A Qualitative StudyDocument21 pagesPerceptions and Experiences of Childhood Vaccination Communication Strategies Among Caregivers and Health Workers in Nigeria: A Qualitative StudyagustinoNo ratings yet
- NCM 112 Assignment on Public Health InformaticsDocument4 pagesNCM 112 Assignment on Public Health InformaticsRoyce Vincent TizonNo ratings yet
- The importance of real-world data to precision medicineDocument4 pagesThe importance of real-world data to precision medicineAngeline JebaNo ratings yet
- Radiation Safety 1Document3 pagesRadiation Safety 1api-632146706No ratings yet
- Systematic Review of Privacy-Preserving Distributed Machine Learning From Federated Databases in Health CareDocument17 pagesSystematic Review of Privacy-Preserving Distributed Machine Learning From Federated Databases in Health CareMessyAnd InStyleNo ratings yet
- Blockchain TechonologyDocument12 pagesBlockchain TechonologySreejith M.G.No ratings yet
- Radiation SafetyDocument4 pagesRadiation Safetyapi-696520673No ratings yet
- Breaking The First Law of Informatics: The Quality and Outcomes Framework (QOF) in The DockDocument5 pagesBreaking The First Law of Informatics: The Quality and Outcomes Framework (QOF) in The DockJosé MªNo ratings yet
- Tizon, R. - Assignment in NCM 112Document4 pagesTizon, R. - Assignment in NCM 112Royce Vincent TizonNo ratings yet
- 15th National Conference For Clinical Research (NCCR)Document40 pages15th National Conference For Clinical Research (NCCR)Institute for Clinical ResearchNo ratings yet
- Privacy Preserving Classification of Clinical Data Using Homomorphic Encryption IJERTCONV3IS12027Document6 pagesPrivacy Preserving Classification of Clinical Data Using Homomorphic Encryption IJERTCONV3IS12027chandravathiNo ratings yet
- BHA-FPX4106 - Nadhirah Lutchminarain - Assignment 3Document19 pagesBHA-FPX4106 - Nadhirah Lutchminarain - Assignment 3Nadhirah De WetNo ratings yet
- Online Healthcare System for Outpatient RecordsDocument42 pagesOnline Healthcare System for Outpatient RecordsFMTech ConsultsNo ratings yet
- Health Information Technology Patient Safety Action & Surveillance PlanDocument50 pagesHealth Information Technology Patient Safety Action & Surveillance PlanS.s. Setyawan PunkrockNo ratings yet
- Ethical Issues of Social Media Usage in HealthcareDocument12 pagesEthical Issues of Social Media Usage in HealthcareFreddy ChopperxNo ratings yet
- A 2020 Vision of Patient CenteredDocument13 pagesA 2020 Vision of Patient CenteredElya Amaliia100% (1)
- Patient Centered Analytics Customizing Treatment Plans Through Data InsightsDocument13 pagesPatient Centered Analytics Customizing Treatment Plans Through Data InsightsEditor IJTSRDNo ratings yet
- Nurs 390 Team Application Project 1 2Document31 pagesNurs 390 Team Application Project 1 2api-621785757No ratings yet
- G7, G8&G9Document9 pagesG7, G8&G9chalie tarekegnNo ratings yet
- Oncology Nursing Trends and Issues 3Document7 pagesOncology Nursing Trends and Issues 3DaichiNo ratings yet
- Personalized Evidence-Based Medicine in Need of High-Quality DataDocument2 pagesPersonalized Evidence-Based Medicine in Need of High-Quality DataJapanese Journal of Gastroenterology and HepatologyNo ratings yet
- 03.state of The Art PS (DR - Nico)Document131 pages03.state of The Art PS (DR - Nico)Devi AmooreaNo ratings yet
- Bank Accounts GuideDocument6 pagesBank Accounts GuideHelloprojectNo ratings yet
- 23rd PSCO ONCO 2019 Peshawar Agenda 1Document8 pages23rd PSCO ONCO 2019 Peshawar Agenda 1Mirza BaigNo ratings yet
- Bfcr182 Safe SedationDocument34 pagesBfcr182 Safe SedationMirza BaigNo ratings yet
- Intimate Examinations and The Use of Chaperones: WWW - Rcr.ac - UkDocument14 pagesIntimate Examinations and The Use of Chaperones: WWW - Rcr.ac - UkMirza BaigNo ratings yet
- bfcr163 Pet-Ct PDFDocument34 pagesbfcr163 Pet-Ct PDFMirza BaigNo ratings yet
- Alarm BSC 2amrDocument1,266 pagesAlarm BSC 2amrswamy137No ratings yet
- Form MGT-6 Return for Beneficial Interest DeclarationDocument8 pagesForm MGT-6 Return for Beneficial Interest DeclarationSameer GahlotNo ratings yet
- Mmi Basic A6 C6Document11 pagesMmi Basic A6 C648884Adam Adam100% (1)
- What is Python? An SEO-Optimized GuideDocument11 pagesWhat is Python? An SEO-Optimized GuidemohitNo ratings yet
- Prepared by Bundala, N.HDocument58 pagesPrepared by Bundala, N.HKanika RelanNo ratings yet
- Document-SAP EWM For Fashion 1.0: 1.general IntroductionDocument3 pagesDocument-SAP EWM For Fashion 1.0: 1.general IntroductionAnonymous u3PhTjWZRNo ratings yet
- Marketing Manager in San Diego CA Resume Eva LangerDocument3 pagesMarketing Manager in San Diego CA Resume Eva LangerevalangerNo ratings yet
- RC Phase Shift Oscillator Using Transistor (BJT) - Circuit & Working - Circuits GalleryDocument3 pagesRC Phase Shift Oscillator Using Transistor (BJT) - Circuit & Working - Circuits GalleryMarkNo ratings yet
- Octonet Catalog Section PDFDocument4 pagesOctonet Catalog Section PDFParasaram SrinivasNo ratings yet
- Contoh Laporan OutputDocument7 pagesContoh Laporan OutputIvan Budi SusetyoNo ratings yet
- 2N Helios IP Vario Installation Manual en 2.3Document79 pages2N Helios IP Vario Installation Manual en 2.3Andrei TryfyNo ratings yet
- Pdms Draft: User Guide Part 2: Drawing AnnotationDocument225 pagesPdms Draft: User Guide Part 2: Drawing AnnotationMakoto TakanoNo ratings yet
- 30 3001 981 Translation+Support+Document+Version+1.94Document34 pages30 3001 981 Translation+Support+Document+Version+1.94Javier Riquelme NovoaNo ratings yet
- Me370 Kdom Lab: Experiment No. 2 Freudenstein'S Method: An Analytical Solution For 4-Bar Synthesis 3-Pt Function GenerationDocument3 pagesMe370 Kdom Lab: Experiment No. 2 Freudenstein'S Method: An Analytical Solution For 4-Bar Synthesis 3-Pt Function GenerationSahilModiNo ratings yet
- The Multiple Document Interface (MDI) : Unit 4Document47 pagesThe Multiple Document Interface (MDI) : Unit 4Manoj BENo ratings yet
- Department of Computer Science and Engineering Obafemi Awolowo University, Ile - Ife Osun StateDocument17 pagesDepartment of Computer Science and Engineering Obafemi Awolowo University, Ile - Ife Osun StateGiwa jelili adebayoNo ratings yet
- Tugas Weekly Report OTIDocument1 pageTugas Weekly Report OTILidiyaNo ratings yet
- SewerCAD QuickStartDocument72 pagesSewerCAD QuickStartMaicol Mena100% (1)
- Lab Report 3 v2Document17 pagesLab Report 3 v2Andy LapianNo ratings yet
- Optimization of Box Section for Double Beam Bridge Crane GirderDocument8 pagesOptimization of Box Section for Double Beam Bridge Crane GirderSomi Khan100% (2)
- Nikon NR-5500 Auto-Refractometer Repair Parts ListDocument47 pagesNikon NR-5500 Auto-Refractometer Repair Parts ListARIF NAQSHBANDINo ratings yet
- Class 8 Math Worksheet 05-CDocument5 pagesClass 8 Math Worksheet 05-CAdam shakilNo ratings yet
- Trắc nghiệm QTHTTTDocument15 pagesTrắc nghiệm QTHTTTTrần Hoàng DiệuNo ratings yet
- Manual Som LG RAD125-ADocument45 pagesManual Som LG RAD125-APortal da Eletrônica100% (1)
- Raster Data Model: A Seminor OnDocument42 pagesRaster Data Model: A Seminor OnAmber Joy TingeyNo ratings yet
- ZKBioSecurity V5000 - 3.0.0 3rd Party API User Manual V1.4 - 20200810Document80 pagesZKBioSecurity V5000 - 3.0.0 3rd Party API User Manual V1.4 - 20200810Oscar GarciaNo ratings yet
- Switched Ethernet vs. Classic EthernetDocument3 pagesSwitched Ethernet vs. Classic EthernetDon WaltonNo ratings yet
- IT Application Areas in CommerceDocument32 pagesIT Application Areas in CommerceRadhika jainNo ratings yet
- Tennis Ball Detection Using Matlab Image ProcessingDocument4 pagesTennis Ball Detection Using Matlab Image ProcessingaaqibNo ratings yet
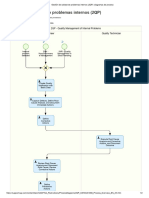
- Gestión de Calidad de Problemas Internos (2QP) - Diagramas de ProcesoDocument2 pagesGestión de Calidad de Problemas Internos (2QP) - Diagramas de ProcesoDiego CincottaNo ratings yet