You might also like
- Data Makes the Difference: The Smart Nurse's Handbook for Using Data to Improve CareFrom EverandData Makes the Difference: The Smart Nurse's Handbook for Using Data to Improve CareNo ratings yet
- Quantitative Article Critique and SummaryDocument8 pagesQuantitative Article Critique and SummaryEmmanuelNo ratings yet
- BSN III 2 Group 3 FinalDocument55 pagesBSN III 2 Group 3 FinalCharinaNo ratings yet
- Child Development Mannualfinal-SinhalaDocument250 pagesChild Development Mannualfinal-SinhalaAshhara FazalNo ratings yet
- Hengameh, 2015Document5 pagesHengameh, 2015aminNo ratings yet
- Clinical Validation of The Nursing Outcome Falls Prevention Behavior in People With StrokeDocument10 pagesClinical Validation of The Nursing Outcome Falls Prevention Behavior in People With Strokeelsy soviantyNo ratings yet
- Training Using Simulation in Internal Medicine Residencies: An Educational PerspectiveDocument3 pagesTraining Using Simulation in Internal Medicine Residencies: An Educational PerspectiveagaetioNo ratings yet
- Documentation 1.en - IdDocument2 pagesDocumentation 1.en - IdAri AzhariNo ratings yet
- Top Research Papers-1Document5 pagesTop Research Papers-1Harsh ThakurNo ratings yet
- Delay EmergencyDocument6 pagesDelay EmergencyKharisma PutraNo ratings yet
- Using Client Outcome Monitoring As A Tool For SupervisionDocument5 pagesUsing Client Outcome Monitoring As A Tool For SupervisionDianaSantiago100% (1)
- Clinical Reasoning Instructor ResourcesDocument17 pagesClinical Reasoning Instructor ResourcesMajid Jafarzadeh100% (1)
- Analysis of Medical Dosimetry Graduates' Level of Preparedness When Entering The WorkforceDocument18 pagesAnalysis of Medical Dosimetry Graduates' Level of Preparedness When Entering The Workforceapi-336793554No ratings yet
- Chapter 6 DiscussionDocument3 pagesChapter 6 DiscussionyughaNo ratings yet
- Introduction:-: Journal HomepageDocument6 pagesIntroduction:-: Journal HomepageIJAR JOURNALNo ratings yet
- Irl FinalDocument17 pagesIrl Finalapi-663098440No ratings yet
- Factors Influencing Decision Making and Its Effect On Intern Students Clinical PerformanceDocument10 pagesFactors Influencing Decision Making and Its Effect On Intern Students Clinical PerformanceTI Journals PublishingNo ratings yet
- Summary of Findings, Conclusions and RecommendationsDocument4 pagesSummary of Findings, Conclusions and RecommendationsIsha JimeneaNo ratings yet
- Chapter 1 Leanne-Rah Inding Bsn3-A - 095557Document8 pagesChapter 1 Leanne-Rah Inding Bsn3-A - 095557Qasra AwaliNo ratings yet
- البحث معدل 1Document27 pagesالبحث معدل 1SiĦãm MỡNo ratings yet
- In The Minds of OSCE Examiners: Uncovering Hidden AssumptionsDocument17 pagesIn The Minds of OSCE Examiners: Uncovering Hidden Assumptionsyacipo evyushNo ratings yet
- Exploration of Knowledge of Adherence To Attitude and Barriers Towardevidencebased Guidelines Ebgs For Prevention of VenDocument7 pagesExploration of Knowledge of Adherence To Attitude and Barriers Towardevidencebased Guidelines Ebgs For Prevention of VenmochkurniawanNo ratings yet
- Sja 18 40Document8 pagesSja 18 40Vis ShyNo ratings yet
- Intensive Care Unit Quality Improvement: A "How-To" Guide For The Interdisciplinary TeamDocument8 pagesIntensive Care Unit Quality Improvement: A "How-To" Guide For The Interdisciplinary TeamJosé Ignacio Cárdenas VásquezNo ratings yet
- ISBAR Communication - Communication Is KeyDocument5 pagesISBAR Communication - Communication Is KeyNaNa HunNo ratings yet
- 1nu350 Sentinel Event Literature Review 1Document5 pages1nu350 Sentinel Event Literature Review 1api-736173301No ratings yet
- White CH 1-6Document76 pagesWhite CH 1-6Rozmine MerchantNo ratings yet
- Final Safety Group Paper490WDocument17 pagesFinal Safety Group Paper490WLYZETTE TERMANNo ratings yet
- Week 6 Assignment: Creating MeasuresDocument7 pagesWeek 6 Assignment: Creating MeasuresDrNo ratings yet
- 2017 - Cabilan & KynochDocument32 pages2017 - Cabilan & KynochazeemathmariyamNo ratings yet
- ISCCM Intensivist GuidelinesDocument28 pagesISCCM Intensivist GuidelinesEsther RaniNo ratings yet
- Utilizing Health Analytics in ImprovingDocument9 pagesUtilizing Health Analytics in ImprovingLikithaNo ratings yet
- Clinical Nursing JudgementDocument6 pagesClinical Nursing Judgementapi-455785477No ratings yet
- Capstone Draft IVDocument13 pagesCapstone Draft IVapi-524151719No ratings yet
- 63afe140741ed Assessment 4 Instructions Informatics and Nursing Sensitive Quality IndicatorsDocument5 pages63afe140741ed Assessment 4 Instructions Informatics and Nursing Sensitive Quality Indicatorskennedy othoroNo ratings yet
- 420 Research PaperDocument12 pages420 Research Paperapi-372913673No ratings yet
- Jurnal Medical Error PDFDocument8 pagesJurnal Medical Error PDFAidha PutryNo ratings yet
- Nursing AuditDocument7 pagesNursing AuditSam ParkNo ratings yet
- En CuestaDocument6 pagesEn CuestaToño VargasNo ratings yet
- Predictors ATLS FailureDocument6 pagesPredictors ATLS FailureKing DonNo ratings yet
- Abstract MSFDocument3 pagesAbstract MSFGreenThumbNo ratings yet
- International Journal of Trend in Scientific Research and Development (IJTSRD)Document16 pagesInternational Journal of Trend in Scientific Research and Development (IJTSRD)Editor IJTSRDNo ratings yet
- Dependency On Laboratory Investigations For Diagnosis by DoctorsDocument3 pagesDependency On Laboratory Investigations For Diagnosis by DoctorsshahzadNo ratings yet
- Sample Thesis FormatDocument35 pagesSample Thesis FormatMichael Erick Valera Virtucio100% (1)
- Clinical Evaluation of Baccalaureate Nursing Students Using SBAR Format: Faculty Versus Self EvaluationDocument5 pagesClinical Evaluation of Baccalaureate Nursing Students Using SBAR Format: Faculty Versus Self EvaluationAngel Joy CatalanNo ratings yet
- Attitudes About Sickness Presenteeism in Medical Training: Is There A Hidden Curriculum?Document9 pagesAttitudes About Sickness Presenteeism in Medical Training: Is There A Hidden Curriculum?faishal azharNo ratings yet
- Integrative Review of The LiteratureDocument21 pagesIntegrative Review of The Literatureapi-507822143No ratings yet
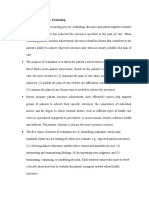
- Key Concepts, Chapter 15, Evaluating: Critically About How Best To Evaluate The Patient's Progress Toward Valued HealthDocument4 pagesKey Concepts, Chapter 15, Evaluating: Critically About How Best To Evaluate The Patient's Progress Toward Valued HealthmsbunnileeNo ratings yet
- For Mbbs For For Recording Practical A and Clinical ActivitiesDocument77 pagesFor Mbbs For For Recording Practical A and Clinical ActivitiesMuhammad Aamir IqbalNo ratings yet
- Individu AzaDocument5 pagesIndividu AzaZachya IslamiaNo ratings yet
- Medical Record Review For FacuDocument7 pagesMedical Record Review For FacuMathilda UllyNo ratings yet
- Assessing Medical Student Documentation Using Simulated Charts in Emergency MedicineDocument6 pagesAssessing Medical Student Documentation Using Simulated Charts in Emergency MedicineRenzo Iván Marín DávalosNo ratings yet
- Module 3-Health Technology, Assessment Study Designs, and EvidencesDocument9 pagesModule 3-Health Technology, Assessment Study Designs, and EvidencesLou CalderonNo ratings yet
- Clinical Nursing JudgmentDocument6 pagesClinical Nursing Judgmentapi-739523749No ratings yet
- Ess 6Document6 pagesEss 6api-582020074No ratings yet
- Title DefenseDocument24 pagesTitle DefenseMary Jane Vega OlescoNo ratings yet
- JournalDocument8 pagesJournalCanam, Allysa F.No ratings yet
- A Paperless' Wall-Mounted Surgical Safety Checklist With Migrated Leadership Can Improve Compliance and Team Engagement (2018)Document5 pagesA Paperless' Wall-Mounted Surgical Safety Checklist With Migrated Leadership Can Improve Compliance and Team Engagement (2018)Teanu Jose Gabrillo TamayoNo ratings yet
- OhnsDocument7 pagesOhnsDaniel AbomaNo ratings yet
- Benefiting From Clinical Experience TheDocument5 pagesBenefiting From Clinical Experience TheSarah Joy BorguetaNo ratings yet
- Glasgow Coma Scale How To Improve and Enhance.9Document3 pagesGlasgow Coma Scale How To Improve and Enhance.9Gun Adi KomaraNo ratings yet
- 22 Dharma RaoDocument4 pages22 Dharma RaoeditorijmrhsNo ratings yet
- Systematic Review of Randomized Controlled Trial Quality in Pediatric Kidney TransplantationDocument10 pagesSystematic Review of Randomized Controlled Trial Quality in Pediatric Kidney Transplantationgede ekaNo ratings yet
- Simple DocDocument2 pagesSimple Docgede ekaNo ratings yet
- Acceptance of The WHO Surgical Safety Checklist Among Surgical Personnel in Hospitals in Guatemala CityDocument5 pagesAcceptance of The WHO Surgical Safety Checklist Among Surgical Personnel in Hospitals in Guatemala Citygede ekaNo ratings yet
- Kanaya Bali DekorDocument1 pageKanaya Bali Dekorgede ekaNo ratings yet
- 04 JorablooDocument6 pages04 Jorabloogede ekaNo ratings yet
- Provisional Broadsheet (Round-II) For Neet-Ug-2023Document175 pagesProvisional Broadsheet (Round-II) For Neet-Ug-2023Đeçeňt BøýNo ratings yet
- MBBS 2020Document346 pagesMBBS 2020Surendra PadhanNo ratings yet
- TS PG Medical Management Quota Admissions List of Colleges: Code Minority College NameDocument1 pageTS PG Medical Management Quota Admissions List of Colleges: Code Minority College NameSunny4288No ratings yet
- Gyne Onco Mission 2022Document5 pagesGyne Onco Mission 2022Dominque RabastoNo ratings yet
- Ai LectureDocument78 pagesAi Lecturesorohmd4No ratings yet
- Show PDFDocument2 pagesShow PDFvallish bharadwajNo ratings yet
- AddressDocument139 pagesAddresspradeeproxNo ratings yet
- Gift-ListDocument40 pagesGift-ListKriti SinhaNo ratings yet
- 1 PBDocument9 pages1 PBMuhammad HikamNo ratings yet
- Sharanjit Purewal - Copy of Action Plan 2019 SeniorsDocument1 pageSharanjit Purewal - Copy of Action Plan 2019 Seniorsapi-438530265No ratings yet
- Phoenix 11 21 GuideDocument7 pagesPhoenix 11 21 GuideJO HN Scuba-rNo ratings yet
- Indore Doctor Data (1) - 1Document34 pagesIndore Doctor Data (1) - 1devNo ratings yet
- Ambedkar Medical College, BangaloreDocument13 pagesAmbedkar Medical College, BangaloreRakeshKumar1987No ratings yet
- Letter From Dean Barbara Bass Update On Residents and Fellows UnionizationDocument3 pagesLetter From Dean Barbara Bass Update On Residents and Fellows Unionizationwamu885No ratings yet
- Camsa 1st Ga Report-2Document74 pagesCamsa 1st Ga Report-2SamuelNo ratings yet
- 5 Combined Provisional Merit List For 1st Online Counselling - PG Medical Courses Under NEET PG-2023 02-08-23Document97 pages5 Combined Provisional Merit List For 1st Online Counselling - PG Medical Courses Under NEET PG-2023 02-08-23Richa GoyalNo ratings yet
- Training Manual On How To Teach Medical EthicsDocument33 pagesTraining Manual On How To Teach Medical EthicsghaiathmeNo ratings yet
- Nepal Medical Colleges Fee 2023-24Document2 pagesNepal Medical Colleges Fee 2023-24brickchattelsNo ratings yet
- Mci Guidelines For ThesisDocument8 pagesMci Guidelines For Thesisginabuckboston100% (2)
- Adv Health JR23 03Document4 pagesAdv Health JR23 03Rahul Agrawal -024No ratings yet
- NEET MDS 2021 Recall 151-200 Questions PDFDocument183 pagesNEET MDS 2021 Recall 151-200 Questions PDFMahima Mishra100% (1)
- Instwiseadm 22122022Document182 pagesInstwiseadm 22122022mr nobodyNo ratings yet
- 421 MS 0049B - JD ClinicalTeachingFellow Obs&Gyne MSDocument13 pages421 MS 0049B - JD ClinicalTeachingFellow Obs&Gyne MSSaquib MohdNo ratings yet
- A Comparative Study of Online Education and Traditional O Ine Education During COVID-19Document19 pagesA Comparative Study of Online Education and Traditional O Ine Education During COVID-19Rahim NensiNo ratings yet
- True MedicineDocument52 pagesTrue MedicineMoga RazvanNo ratings yet
- G.R. No. 78164 July 31, 1987 - TERESITA TABLARIN, ET AL. v. ANGELINA S. GUTIERREZ: July 1987 - Philipppine Supreme Court DecisionsDocument31 pagesG.R. No. 78164 July 31, 1987 - TERESITA TABLARIN, ET AL. v. ANGELINA S. GUTIERREZ: July 1987 - Philipppine Supreme Court DecisionsJeunice VillanuevaNo ratings yet
- Tutorials: An Effective and Interactive Method of Teaching Undergraduate Medical StudentsDocument3 pagesTutorials: An Effective and Interactive Method of Teaching Undergraduate Medical StudentsKumar BhasinNo ratings yet
- JC To CoverDocument2 pagesJC To CoverNogra Carl0% (1)