0% found this document useful (0 votes)
59 views4 pagesUnderstanding Atopic Dermatitis: Causes & Treatments
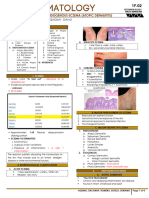
1) Atopic dermatitis is a chronic eczema caused by an atopic condition like asthma or allergies. It is characterized by dry, scaly patches that are itchy.
2) The symptoms vary depending on age. In infants it starts as redness and scales on the face and scalp, spreading to the body. In children it causes dry, lichenified plaques on elbows and knees. In adolescents and adults the plaques enlarge and spread over the body.
3) The causes involve both a defective skin barrier and immune abnormalities like high IgE levels that make the skin vulnerable to irritation and itchy eczema. Topical steroids and immunosuppress
Uploaded by
Hafiz AzizCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
59 views4 pagesUnderstanding Atopic Dermatitis: Causes & Treatments
1) Atopic dermatitis is a chronic eczema caused by an atopic condition like asthma or allergies. It is characterized by dry, scaly patches that are itchy.
2) The symptoms vary depending on age. In infants it starts as redness and scales on the face and scalp, spreading to the body. In children it causes dry, lichenified plaques on elbows and knees. In adolescents and adults the plaques enlarge and spread over the body.
3) The causes involve both a defective skin barrier and immune abnormalities like high IgE levels that make the skin vulnerable to irritation and itchy eczema. Topical steroids and immunosuppress
Uploaded by
Hafiz AzizCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd