Professional Documents
Culture Documents
Multiple Myeloma Diagnosis and
Uploaded by
Jorge BarcenasOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Multiple Myeloma Diagnosis and
Uploaded by
Jorge BarcenasCopyright:
Available Formats
Review Article
Multiple Myeloma: Diagnosis and
Orthopaedic Implications
Abstract
Thomas J. Scharschmidt, MD Multiple myeloma is a hematologic malignancy that commonly
Joshua D. Lindsey, MD affects the skeletal system. The disease is primarily managed
medically with chemotherapeutic agents. Pathologic fractures are
Pamela S. Becker, MD, PhD
common in patients with diagnosed and undiagnosed disease. The
Ernest U. Conrad, MD number of patients diagnosed with multiple myeloma is increasing,
as is the incidence of associated pathologic fractures. Novel
chemotherapeutic agents and radiation therapy protocols have
been used to extend the average life span of patients with this
disease. Various methods that allow for restoration of function and
pain reduction can be used to stabilize and manage fractures
associated with multiple myeloma. The orthopaedic surgeon and
oncology team must work together to develop an individualized
treatment plan to improve patient quality of life and provide pain
relief.
M ultiple myeloma is a hematog-
enous malignancy of mono-
clonal plasma cells that typically
ings are associated with poor
outcome.6 However, the specific
mechanism of the transition of a
presents with pain, pathologic frac- plasma cell to a population of malig-
ture, recurrent infection, and/or fa- nant monoclonal plasma cells is
tigue. The annual incidence of newly largely unknown (Figure 1).
diagnosed cases in the United States Several diagnoses associated with
is 3 to 4 per 100,000 people.1 The multiple myeloma are considered in
median age at diagnosis is 65 years, the spectrum of disease. These in-
with a slight male predilection. Mul- clude symptomatic myeloma, asymp-
tiple myeloma accounts for approxi- tomatic or smoldering myeloma,
mately 1% of all malignant diseases, monoclonal gammopathy of unde-
and median survival is approxi- termined significance, nonsecretory
mately 50 months after diagnosis.2,3 myeloma, and solitary plasmacy-
From the Department of toma2,3,7,8 (Table 1).
Orthopaedics, Ohio State University
Symptomatic myeloma represents
College of Medicine, Columbus, OH
(Dr. Scharschmidt), the Department Spectrum of Disease the classic definition of multiple my-
of Orthopaedics and Sports eloma. The diagnosis is typically
Medicine (Dr. Lindsey and Plasma cells are of B-lymphocyte lin- made after the patient presents with
Dr. Conrad), and the Division of eage. These cells are responsible for symptoms such as unexplained ane-
Hematology (Dr. Becker), University
producing antibodies after exposure mia, renal failure, bone pain, infec-
of Washington Medical Center,
Seattle, WA. to an antigen. Several mutations tion, and hypercalcemia.1,3 Serum
have been identified in association and/or urine electrophoresis results
J Am Acad Orthop Surg 2011;19:
410-419 with multiple myeloma; the most demonstrate a monoclonal protein
common are mutation of chromo- level (ie, M spike) that represents the
Copyright 2011 by the American
Academy of Orthopaedic Surgeons. some 14q32 and deletion of chromo- antibody produced by the tumor
some 13.4-6 These cytogenetic find- cells. Immunoglobulin (Ig) G is the
410 Journal of the American Academy of Orthopaedic Surgeons
Thomas J. Scharschmidt, MD, et al
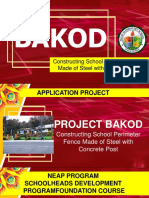
Figure 1 detected on serum and/or urine elec- mediator of myeloma bone disease.
trophoresis, and evidence of end- Knowledge of this pathologic pro-
organ damage (eg, hypercalcemia, cess has led to increased use of
renal insufficiency, anemia, bone le- diphosphonates to treat patients
sions, more than two severe infec- with multiple myeloma.
tions per year, amyloidosis, hypervis-
cosity syndrome).2,3,7,8
Clinical Presentation
Clinical presentation of multiple my-
Myeloma Bone Disease
eloma ranges from asymptomatic,
Lytic bone disease is a hallmark of mul- with incidental discovery, to symp-
Photomicrograph demonstrating tiple myeloma, and a substantial per- tomatic, with severe life-threatening
typical multiple myeloma histology, anemia, infection, or disabling bone
with monoclonal proliferation of centage of patients develop pathologic
plasma cells (hematoxylin-eosin, fractures.9 Bone resorption occurs as pain. Fatigue, bone pain, and recur-
magnification ×200). rent infections are the most common
the result of osteoclastic stimulation
presenting complaints. Multiple end
and activity. Osteoblastic activity de-
organs can be affected by myeloma,
most common antibody detected, but creases, as evidenced by low levels of
which explains the wide spectrum of
any of the subtypes (ie, IgM, IgE, alkaline phosphatase and osteocal-
presenting symptoms; these symp-
IgA) may be present. The abnormal cin.10 The uncoupling of osteoclastic
toms (ie, hypercalcemia, renal insuf-
proteins found in urine (ie, Bence and osteoblastic activity leads to
ficiency, anemia, and bone lesions)
Jones) are composed of the free light overall bone loss.
are often referred to by the abbrevia-
chains that are excreted through the The pathophysiology of myeloma
tion “CRAB.”1,3
kidney.3 bone disease is primarily driven by
A skeletal survey is performed to osteoclastic stimulation by malignant
evaluate for the presence of bony le- cells. The osteoclast, not the my- Staging
sions. The serum calcium level is eloma cell itself, is responsible for
evaluated; it is often elevated. Bone bone destruction. Myeloma cells ad- The Durie-Salmon system has tradi-
marrow aspirate is evaluated to mea- here to bone marrow stromal cells tionally been used to stage multiple
sure the percentage of plasma cells. and stimulate the production of re- myeloma. This complex classifica-
Quantitative Ig assay should be ob- ceptor activator of nuclear factor-κ B tion takes into account the quantity
tained to determine the extent of im- ligand (RANKL) and other pro- of monoclonal proteins in the blood
munoparesis. Kidney function tests osteoclastic mediators (eg, macro- or urine, hemoglobin level, serum
should be performed; the results may phage colony-stimulating factor, calcium level, findings on skeletal
be altered as the result of protein de- interleukin-6, interleukin-11, tumor survey, and renal function as deter-
position. The β-2 microglobulin necrosis factor).11 The production of mined by serum creatinine level.12
(β2M) level, which has been linked osteoprotegerin, which competes Although the Durie-Salmon classi-
to overall prognosis, should be mea- with receptor activator of nuclear fication is still used, it is being super-
sured, as well. The diagnostic criteria factor-κ to bind to RANKL as a seded by the much simpler Interna-
for symptomatic myeloma include decoy receptor, is also suppressed, re- tional Staging System (ISS), which
the presence of all of the following: sulting in further osteoclast activa- was published in 2005 by the Inter-
clonal plasma cells >10% on bone tion. Thus, the RANKL/osteo- national Myeloma Working Group.13
marrow biopsy, monoclonal protein protegerin pathway is the primary The ISS is based on β2M and albu-
Dr. Becker or an immediate family member serves as a board member, owner, officer, or committee member of the National
Comprehensive Cancer Network; serves as a paid consultant to or is an employee of Alder Biopharmaceuticals; has received
research or institutional support from Amgen, Genzyme, Millenium: The Takeda Oncology Company, and Celgene; and has stock or
stock options held in Forest Laboratories. Dr. Conrad or an immediate family member serves as a paid consultant to or is an
employee of Zimmer; serves as an unpaid consultant to Stryker; has received research or institutional support from Zimmer; and has
received nonincome support (such as equipment or services), commercially derived honoraria, or other non-research–related funding
(such as paid travel) from Northwest Tissue Services/Puget Sound Blood Center. Neither of the following authors nor any immediate
family member has received anything of value from or owns stock in a commercial company or institution related directly or indirectly
to the subject of this article: Dr. Scharschmidt and Dr. Lindsey.
July 2011, Vol 19, No 7 411
Multiple Myeloma: Diagnosis and Orthopaedic Implications
Table 1
Diagnosis and Management of Multiple Myeloma2,3,7,8
Diagnosis Diagnostic Criteria Management Prognosis
Symptomatic >10% clonal plasma cells present Transplant candidates: autologous ISS stage I, 62 mo; stage II, 44 mo;
myeloma on bone marrow biopsy stem cell transplantation with stage III, 29 mo
Monoclonal protein detected on induction chemotherapy
serum and/or urine Nontransplant candidates: chemo-
electrophoresis therapy
Evidence of end-organ damage
(eg, hypercalcemia, renal insuffi-
ciency, anemia, bone lesions,
>2 severe infections per year,
amyloidosis, hyperviscosity syn-
drome)
Asymptomatic (ie, Same as symptomatic myeloma, Routine surveillance (every 2-3 mo Once the patient progresses to
smoldering) but without evidence of end- by an oncologist) symptomatic myeloma, the prog-
myeloma organ involvement nosis is the same as that of
symptomatic myeloma
Monoclonal gammop- Asymptomatic, often discovered Annual electrophoresis for surveil- Prognosis is determined after pro-
athy of undeter- incidentally lance gression to symptomatic my-
mined significance Monoclonal band <30 g/L, plasma eloma. Approximately 10% pro-
cells <10% gress to symptomatic myeloma.
Nonsecretory Same as symptomatic myeloma, Transplant candidates: autologous ISS stage I, 62 mo; stage II, 44 mo;
myeloma except that plasma cells do not stem cell transplantation with in- stage III, 29 mo
produce protein, so electrophore- duction chemotherapy
sis is negative for protein Nontransplant candidates: chemo-
therapy
Plasmacytoma Solid tumor composed of plasma Radiation, surveillance Prognosis is determined after pro-
cells in bone or soft tissue gression to symptomatic my-
eloma. Approximately10%–15%
progress to symptomatic my-
eloma.
ISS = International Staging System
min levels. β2M is part of the major ease is characterized by the presence
histocompatibility complex protein Imaging of 5 to 20 focal bone lesions and/or
class that is present in all nucleated moderate diffuse spine disease visible
In the patient with suspected multi-
cells. β2M levels can be elevated in on MRI. In stage III disease, >20 fo-
ple myeloma, a radiographic skeletal
patients with renal disease, lym- cal bone lesions and/or severe diffuse
survey should be performed concur-
phoma, and other disease processes; spine disease is visible on MRI.
rently with bone marrow aspiration
therefore, the ISS should be applied
only to patients who match the crite- and either serum or urine electropho- Radiography
ria for the diagnosis of multiple my- resis. The survey should be scruti- Plain radiographs are the standard of
eloma. nized for multiple lytic lesions. The care for evaluation of persons with
ISS stage I disease is defined by a number of lytic bone lesions is one myeloma. A survey of the appendicu-
β2M level <3.5 mg/L and serum al- criterion in the Durie-Salmon staging lar skeleton, spine, pelvis, and skull
bumin level ≥3.5 g/dL. Patients with system. In 2003, the original system should be performed in persons with
stage II disease have β2M levels be- was updated to incorporate MRI suspected myeloma. However, le-
tween 3.5 and 5.4 mg/L. Stage III findings and was renamed Durie- sions are not evident on plain radio-
disease is characterized by β2M level Salmon PLUS.14 In the updated sys- graphs until approximately 50%
≥5.5 mg/L. The ISS correlates well tem, stage I disease is characterized bone destruction has occurred.2 Even
with average reported survival rates: by the presence of zero to four focal so, approximately 80% of patients
stage I, 62 months; stage II, 44 bone lesions and/or mild diffuse with multiple myeloma have positive
months; and stage III, 29 months.13 spine disease on MRI. Stage II dis- radiographic findings at presenta-
412 Journal of the American Academy of Orthopaedic Surgeons
Thomas J. Scharschmidt, MD, et al
Figure 2 evaluation of the cross-sectional Schirrmeister et al19 reported that
anatomy of the lesion, which is im- FDG PET had a sensitivity of 92.7%
portant for gauging the integrity of in identifying radiographically os-
the cortical bone and predicting the teolytic lesions in 23 patients. In 14
risk of pathologic fracture. Although patients, lesions that were not appar-
mechanical pain may be the best in- ent radiographically were detected
dicator of an impending fracture, in- on FDG PET.
volvement of >50% of the cortical PET has been demonstrated to be
bone visible on CT has traditionally more sensitive than radiographs in
been one of the criteria used for rec- screening and diagnosing myeloma.
ommending prophylactic fixation In fact, Lütje et al20 suggested that
versus radiation therapy.16 Any pa- FDG PET used in combination with
tient who may have an impending low-dose CT can replace conven-
fracture that is not obvious on plain tional radiographs as the standard of
radiographs should be evaluated care. Most large centers now use
with CT through the lesion. CT- FDG PET as part of the initial stag-
guided biopsy is used for tissue diag- ing and in assessing patient response
nosis in the setting of inconclusive to treatment.18,21 FDG PET also
results on serum or urine electropho- should be considered in patients with
resis. a diagnosis of solitary plasmacytoma
because it may uncover additional
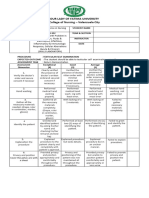
AP radiograph of a hip Nuclear Medicine Studies sites of disease. In a study of 15 pa-
demonstrating multiple lytic tients with known plasmacytoma
Technetium-based bone scans rely on
punched-out lesions in a patient who underwent FDG PET for stag-
with multiple myeloma. These an osteoblastic response for uptake
lesions typically measure <2 cm of the radiopharmaceutical agent. ing, additional lesions were found in
and lack reactive bone around the Because multiple myeloma is primar- 5 patients, which resulted in treat-
defect.
ily driven by osteoclastic activity and ment modification for 4 patients.22
is a disease of bone resorption, bone
scan tends to be unreliable, and the MRI
tion.15 Typical myeloma lesions are extent of disease can be underesti- Indications for MRI in patients with
small (average, 20 mm) and lytic, mated. Hubner et al17 compared multiple myeloma are expanding.
with a sharp zone of transition and bone scans with plain radiographs MRI appears to be more sensitive
lack of reactive bone15 (Figure 2). for the evaluation of bone lesions. and specific than radiography in
Four distinct forms of myeloma have Uptake occurred on the bone scan in identifying bone marrow lesions, es-
been identified radiographically: soli- only 44% of radiographically abnor- pecially in the pelvis and spine.23 On
tary plasmacytoma, diffuse disease, mal areas, and findings were normal T1-weighted spin-echo images, a le-
diffuse osteopenia, and sclerosing in 48% of these lesions.2,17 In gen- sion appears as a hypointense area
myeloma.2 Plain radiographs are the eral, lesions with uptake on bone on a background of hyperintense
most widely used standardized test scan are the result of a complication marrow. T2-weighted spin-echo se-
for the evaluation of impending and of myeloma, such as insufficiency or quences reveal hyperintense focal im-
pathologic fractures associated with pathologic fracture. Therefore, a ages relative to the hypointense mar-
multiple myeloma. bone scan is not recommended as row (Figure 3). Diffuse involvement
part of routine staging in persons presents as general hyperintensity
CT with multiple myeloma. compared with the surrounding mus-
CT is helpful in defining the extent The use of fludeoxyglucose F 18 culature.15
of lytic bone lesions that are poorly positron emission tomography (FDG Several authors have recommended
visualized radiographically. Common PET) is gaining in popularity in MRI of the entire appendicular skel-
findings include punched-out lytic le- many areas of oncology for early de- eton, pelvis, and spine at the time a
sions, expansile lesions with soft- tection, staging, and monitoring of patient is diagnosed with multiple
tissue masses, pathologic fractures, diseases such as multiple myeloma.18 myeloma.8,21,23 Some authors suggest
and osteosclerosis.2 CT also allows In a recent series of 43 patients, that initially obtaining an MRI may
July 2011, Vol 19, No 7 413
Multiple Myeloma: Diagnosis and Orthopaedic Implications
Figure 3 Figure 4
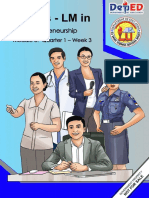
Sagittal T2-weighted spin-echo
magnetic resonance image
demonstrating a large sacral lesion
in a patient with multiple myeloma.
In this image, all lesions have
hyperintense signal characteristics.
obviate the need for additional stud-
ies in patients in whom stage III
disease is apparent on that MRI sur-
vey.21 Findings suggestive of my-
eloma include an expansile focal
mass, multiple focal masses in the
appendicular skeleton, diffuse mar-
Treatment algorithm for newly diagnosed myeloma. * ≥12 months of therapy
row involvement, and multiple com- and stable disease for ≥2 months. (Adapted with permission from Kyle RA,
pression fractures in the patient with Rajkumar SV: Multiple myeloma. N Engl J Med 2004;351[18]:1860-1873.)
no known malignancy.
MRI or FDG PET should also be
Initial Therapy
obtained in the patient with sus- Medical Management
pected solitary plasmacytoma. Addi- Nontransplant Candidate
tional lesions have been reported in Management of myeloma addresses Patients with medical comorbidities,
up to one third of cases evaluated us- plasma cell proliferation and symp- of advanced age, or in poor physical
ing whole-body MRI.23 Patient treat- toms secondary to it. Treatment of condition are not candidates for
ment is affected by the number of le- patients with monoclonal gammop- transplantation. These patients are
sions present. athy of undetermined significance or treated with oral melphalan and
MRI also may be used to monitor asymptomatic myeloma consists of prednisone in combination with ei-
response to treatment because it can annual surveillance to monitor for ther thalidomide or bortezomib1,26
show reduction in or resolution of le- transformation to symptomatic my- (Figure 4). The cycles of melphalan
sions identified on initial imaging. eloma. There is no evidence that plus prednisone reduce the collection
Resolution of the bone marrow to a early management of asymptomatic of peripheral blood stem cells, but in
normal pattern is associated with a myeloma improves survival.25 Initial older patients (ie, >65 years), they
better prognosis and longer remis- therapy for symptomatic myeloma is also reduce the severity of toxic side
sion.21,24 Most centers now favor determined by whether the patient is effects. Better response rates are seen
PET-CT to MRI for evaluating pa- a candidate for autologous stem cell with more aggressive regimens (ie,
tients with multiple myeloma. transplantation1,3 (Figure 4). lenalidomide-dexamethsone or tha-
414 Journal of the American Academy of Orthopaedic Surgeons
Thomas J. Scharschmidt, MD, et al
lidomide-dexamethasone); however, of autologous stem cells, followed by therapy, such as anemia and neurop-
no survival benefit has been shown.1 high-dose melphalan chemotherapy athy. Adjuvant agents and processes,
and infusion of stem cells.1 Tandem including diphosphonates, growth
Transplant Candidate sequential autologous (ie, double- factors, transfusion, and vitamin
Transplant candidates undergo in- auto) transplants have demonstrated supplements, can be used to manage
duction therapy consisting of dexa- an advantage in patients with resid- these complications (Table 2).
methasone combined with thalido- ual myeloma following the first
mide, lenalidomide, or bortezomib.1,3
transplant.3,27
Combinations include lenalidomide
Minimal myeloablative (ie, mini- Orthopaedic
and dexamethasone; bortezomib and Considerations
allo) regimens were developed in re-
dexamethasone; bortezomib, thalid-
sponse to substantial mortality fol- The orthopaedic surgeon may be
omide, and dexamethasone; and
lowing high-dose melphalan and consulted to perform a biopsy for
bortezomib, lenalidomide, and dex-
high-dose total body irradiation with
amethasone. Approximately 70% to initial diagnosis, provide recommen-
allogeneic stem cell transplantation.
90% of patients respond to initial dations for nonsurgical care, per-
A combination of autologous trans-
therapy.1 Side effects include myelo- form prophylactic fixation of im-
plant followed by mini-allo trans-
suppression, thrombosis, gastrointes- pending fractures, or stabilize
plant has been shown to be success-
tinal effects (eg, infection, diarrhea), pathologic fractures in the patient
ful.28 In one study, 6 of 13 patients
and neuropathy. Most of these side with myeloma bone disease. Typi-
who showed response to initial che-
effects are reversible. cally, a patient presents with an im-
motherapy and who achieved partial
pending or pathologic fracture with
or complete remission following the
Autologous and Allogeneic no prior diagnosis of myeloma. In
combined procedure were event-free
Stem Cell Transplantation the patient with a bone lesion and
at 2-year follow-up.29 Maintenance
Autologous stem cell transplantation unknown primary malignancy, the
therapy with interferon alpha or
involves transplantation of the pa- workup includes radiographs of the
prednisone can be considered after
tient’s own stem cells after chemo- entire bone; bone scan; MRI of the
autologous or allogeneic stem cell
therapy. This procedure is not cura- extremity; CT of the chest, abdomen,
transplant in an effort to prolong the
tive. However, it has been shown to and pelvis; complete blood count; se-
time to progression; however, con-
increase disease-free survival by 2 to rum and/or urine electrophoresis;
troversy persists regarding the bene-
3 years.3 Candidates are selected prostate-specific antigen in men; and,
fit of this therapy.1
based on age, performance status (ie, in women, a breast examination or
measure of disease burden on overall mammogram. In a prospective study
Salvage Therapy
patient activities), and evidence of of 40 patients with skeletal metasta-
preserved organ function. In younger Eventual relapse after treatment is ses of unknown origin who were
transplant candidates (ie, aged <65 the natural history of multiple my- evaluated using this strategy, the pri-
years), combinations of induction eloma. With relapse that occurs >6 mary site of the malignant tumor
chemotherapeutic drugs are recom- months after prior therapy, the was identified in 34 patients
mended. These drugs are not toxic to potential exists for a therapeutic re- (85%).31
the hematopoietic cells and do not sponse to the initial therapy regi- When the electrophoresis is posi-
impair the ability to collect adequate men.30 Regimens for relapsed my- tive, radiographic bone survey and
numbers of peripheral blood stem eloma that have been studied and bone marrow biopsy are performed
cells. Given the multiple treatments approved by the US FDA include for staging. However, no further bi-
available and the lack of consensus lenalidomide and dexamethasone, opsy of the lesion is required for di-
regarding which is most effective, pa- bortezomib and dexamethasone, and agnosis. Biopsy is required in some
tients are encouraged to enroll in bortezomib and liposomal doxoru- cases, such as in the patient with sus-
clinical trials in an effort to deter- bicin. pected plasmacytoma and when elec-
mine best practices. trophoresis is not obtained. Biopsy
In general, patients are treated Additional Adjuvant Agents must be done carefully because my-
with a chemotherapy regimen for Patients with multiple myeloma may eloma lesions can be very vascular,
several months until maximal re- suffer from conditions related to the and there is a risk of substantial
sponse is achieved, after which they complexity of the disease process blood loss. This should also be taken
undergo mobilization and collection and to complications associated with into account during preplanning for
July 2011, Vol 19, No 7 415
Multiple Myeloma: Diagnosis and Orthopaedic Implications
Table 2 Dexamethasone is used in many regi-
mens, and a stress dose of steroids
Adjuvant Agents for Managing Complications Associated With Multiple
Myeloma Therapy may be warranted at the time of sur-
gery.
Category Agent Indications Patients with a malignant diagnosis
Diphosphonate Pamidronate, zoledronic Evidence of bone loss are at increased risk of thromboem-
acid bolic disease, and chemotherapy in-
Growth factor Granulocyte colony–stimu- Neutropenia associated with creases this risk further, to sevenfold
lating factor agents such as bortezomib, that of the general population.32 As
lenalidomide, or combination
such, these patients are considered to
therapies
be at highest risk of deep vein throm-
Epoetin α, darbepoietin Patients with renal insufficiency
with subsequent erythropoietin bosis and pulmonary embolism, and
production may benefit from they are typically treated in accor-
supplementation. dance with the American College of
Transfusion — Treatment-acquired anemia and Chest Physicians guidelines on thera-
thrombocytopenia may require
peutic heparin (international normal-
red cell and/or platelet transfu-
sion. ized ratio, 2 to 3) or low-molecular-
Vitamin supplement Pyridoxine Vitamin supplements may be weight heparin.33 Anticoagulation
and other medica- helpful in preventing drug- therapy may need to be stopped and
tions related peripheral neuropathy. coagulopathies corrected preopera-
Thalidomide and bortezomib in
particular are associated with
tively, with resumption of anticoagu-
neuropathy. lation immediately postoperatively.
Gabapentin, pregabalin Painful neuropathy In patients with multiple myeloma,
surgical indications are typically lim-
ited to management of impending or
intramedullary or open procedures. who is being considered for bone pathologic fracture. A substantial
Blood type and crossmatch should be marrow transplant. In this scenario, percentage of patients with multiple
obtained prior to either type of sur- an aggressive surgical approach pre- myeloma develop pathologic frac-
gery. transplant may be considered. If such tures.9 Basic principles of surgery for
The orthopaedic surgeon may be a lesion were to progress and result patients with metastatic disease
asked to evaluate a painful bone in a fracture during the transplant, should be followed, including preop-
lesion in a patient with known my- the patient would be at risk of a long erative imaging of the entire involved
eloma to determine whether prophy- delay prior to surgical fixation. Were bone, achieving an immediately sta-
lactic surgical stabilization is war- such a fracture to occur in a weight- ble and durable construct, and post-
ranted. Not all bone lesions are bearing bone, requiring a long period operative radiation therapy.16,34,35
prone to fracture, and several factors of bed rest, the immunocompro- Overall patient prognosis and life ex-
should be considered when deciding mised patient would be at risk of pectancy should be considered prior
on appropriate treatment. pneumonia, pressure sores, and gen- to any surgical intervention.
Pain can be produced by the tumor eral deconditioning. For impending fracture or a pain-
itself or by mechanical weakening of In the patient with myeloma, sev- ful lesion that is unresponsive to ra-
the bone. When the tumor is the eral medical factors must be consid- diation therapy, stabilization surgery
cause of pain, the lesion frequently ered before proceeding with surgery. is typically recommended when life
responds to radiation therapy. Non- Many newly diagnosed patients are expectancy is >3 months. This allows
surgical management also should be hypercalcemic, and this condition ample time for postoperative recov-
considered for lesions in non–weight must be managed prior to surgical ery and achievement of beneficial
bearing areas (eg, upper extremity, il- intervention. Consultation with the pain relief. For the patient whose life
iac wing) in which surgical manage- medical oncologist is essential be- expectancy is <3 months, palliative
ment could delay systemic care. cause many chemotherapeutic agents treatment should be discussed with
Another important consideration is cause myelosuppression and may the patient and family. When surgery
a lesion that does not meet criteria cause a nadir at various times after is chosen, as much of the involved
for surgical stabilization but is lo- administration of the drug; this bone as possible is stabilized, typi-
cated in a high-risk area in a patient could affect optimal surgical timing. cally with intramedullary fixation, to
416 Journal of the American Academy of Orthopaedic Surgeons
Thomas J. Scharschmidt, MD, et al
Figure 5 Figure 6
AP radiograph demonstrating
humeral stabilization with an A, Preoperative AP radiograph of the hip demonstrating pathologic fracture
intramedullary implant in a patient through a myeloma lesion. B, Postoperative AP radiograph demonstrating a
with a myeloma lesion in the stable, durable construct achieved with a modular proximal femoral
humerus. prosthesis.
avoid creating new stress risers in intact, we prefer to perform curet- years after the procedure.39 MRI
pathologic bone (Figure 5). For a tage of the lesion and stabilize it with should be done preoperatively to as-
large defect, curettage can be per- polymethylmethacrylate cement and sess for extraosseous disease. In the
formed, and the bone can be stabi- modified Harrington pin fixation. If patient with considerable soft-tissue
lized with polymethylmethacrylate the subchondral plate is violated by involvement, radiation therapy to
cement around the intramedullary tumor extension, complex total hip the area before stabilization may be
device. reconstruction with an acetabular
helpful.
For a periarticular lesion, a custom cage is performed. Internal or exter-
Neural compression or more ex-
or megaprosthesis can be used, with nal hemipelvectomy can be consid-
tensive spinal bony involvement that
the goal of achieving an immediately ered in the patient with intractable
is not amenable to a percutaneous
durable construct that allows early pain.
procedure is relatively rare, given the
mobilization36 (Figure 6). Good func- Spinal compression fractures have
sensitivity of the disease to radiation
tional results and pain relief can be been identified in >40% of patients
therapy. In patients who present with
expected.36,37 The surgeon should with newly diagnosed myeloma.2 In
painful lesions, percutaneous verte- either neural compression or exten-
avoid using press-fit implants and
constructs that rely on bony in- broplasty has proved to be effective sive bony involvement, effective
growth. in alleviating pain.38 In that study, all management typically consists of spi-
The periacetabular region is a com- 10 patients with multiple myeloma nal cord decompression and stabili-
mon site of myeloma lesions. Periac- reported mild or moderate pain re- zation of the vertebral column
etabular lesions often present with lief. These interventions allow imme- through an anterior, a posterior, or a
large cavities and are painful as a re- diate improvement in quality of life combined approach. Although these
sult of their presence in a weight- following an outpatient procedure or procedures are extensive, they result
bearing area. Few appealing surgical a short hospital stay (80% reported in significant improvement in patient
interventions exist, given the com- pain relief within 7 days of the pro- quality of life and pain reduction,
plex anatomy of the bony pelvis. If cedure).38 In most patients, pain re- along with stabilization or improved
the acetabular subchondral plate is lief can be expected to last up to 2 neurologic function.39
July 2011, Vol 19, No 7 417
Multiple Myeloma: Diagnosis and Orthopaedic Implications
fests in various ways. Bony pain and Transplant 1999;24(5):497-503.
Radiation Therapy pathologic fracture are among the 7. Kyle RA, Rajkumar SV: Monoclonal
most common presentations. In the gammopathy of undetermined
External beam radiation therapy is a significance and smouldering multiple
mainstay of treatment in the patient past decade, advances in treatment myeloma: Emphasis on risk factors for
with myeloma bone disease.40 It is have led to improved outcomes in progression. Br J Haematol 2007;139(5):
730-743.
used as an antimyeloma therapy as patients with multiple myeloma, in-
cluding event-free and overall sur- 8. Walker R, Barlogie B, Haessler J, et al:
well as a palliative treatment method Magnetic resonance imaging in multiple
in patients with incurable disease. vival. As a result, more patients are myeloma: Diagnostic and clinical
Radiation therapy alone has the po- presenting with orthopaedic manifes- implications. J Clin Oncol 2007;25(9):
1121-1128.
tential to be curative in patients with tations of the disease. Thus, ortho-
9. Lentzsch S, Ehrlich LA, Roodman GD:
solitary plasmacytoma.41 However, it paedic surgeons need to understand
Pathophysiology of multiple myeloma
is typically used for palliative pain the basic pathophysiology of the dis- bone disease. Hematol Oncol Clin North
relief in patients with symptomatic ease and the appropriate manage- Am 2007;21(6):1035-1049, viii.
lesions. Pain relief is typically ment of impending and pathologic 10. Vejlgaard T, Abildgaard N, Jans H,
fractures. Nielsen JL, Heickendorff L: Abnormal
achieved with a dose of approxi-
bone turnover in monoclonal
mately 3,000 cGy administered in 10 gammopathy of undetermined
to 15 fractions.42 significance: Analyses of type I collagen
Other indications for radiation References telopeptide, osteocalcin, bone-specific
alkaline phosphatase and propeptides of
therapy include impending or patho- type I and type III procollagens. Eur J
Evidence-based Medicine: Levels of Haematol 1997;58(2):104-108.
logic fracture, spinal cord compres-
evidence are described in the table of 11. Brenner H, Gondos A, Pulte D: Expected
sion, and other local neurologic
contents. In this article, references 4 long-term survival of patients diagnosed
problems caused by tumor. Patients with multiple myeloma in 2006-2010.
and 26 are level I studies. References
who undergo surgical fixation or sta- Haematologica 2009;94(2):270-275.
5, 7, 11, 19, 21, 24, 27, 29, 38, 40,
bilization of an active lesion should 12. Durie BG, Salmon SE: A clinical staging
and 41 are level II studies. Reference system for multiple myeloma:
be treated with adjuvant radiation to
35 is a level IV study. References 1-3, Correlation of measured myeloma cell
the surgical field to decrease local re- mass with presenting clinical features,
8, 9, 16, 25, and 39 are level V ex-
currence of the disease. Adjuvant ra- response to treatment, and survival.
pert opinion. Cancer 1975;36(3):842-854.
diation is not used in persons with
mechanical failure of the bone, as is References printed in bold type are 13. Greipp PR, San Miguel J, Durie BG,
those published within the past 5 et al: International staging system for
seen in those who have responded multiple myeloma. J Clin Oncol 2005;
well to chemotherapy and who have years. 23(15):3412-3420.
residual lytic cavities. 1. Rajkumar SV, Palumbo A: Management 14. Durie BG: The role of anatomic and
Radiotherapeutic agents (eg, stron- of newly diagnosed myeloma. Hematol functional staging in myeloma:
Oncol Clin North Am 2007;21(6):1141- Description of Durie/Salmon plus
tium 89) have been described as a 1156. staging system. Eur J Cancer 2006;
palliative treatment in the patient 42(11):1539-1543.
2. Angtuaco EJ, Fassas AB, Walker R, Sethi
with intractable bone pain.2 Re- R, Barlogie B: Multiple myeloma: 15. Collins CD: Multiple myeloma. Cancer
sponse to these adjuvants is depen- Clinical review and diagnostic imaging. Imaging 2004;4 Spec No A:S47-S53.
Radiology 2004;231(1):11-23.
dent on an osteoblastic response and 16. Frassica FJ, Frassica DA: Metastatic
may not be effective in a purely os- 3. Kyle RA, Rajkumar SV: Multiple bone disease of the humerus. J Am Acad
myeloma. N Engl J Med 2004;351(18): Orthop Surg 2003;11(4):282-288.
teoclastic scenario. Thus, technetium 1860-1873.
17. Hubner KF, Andrews GA, Hayes RL,
bone scan should be obtained prior 4. Avet-Loiseau H: Role of genetics in Poggenburg JK Jr, Solomon A: The use
to radiation therapy to identify the prognostication in myeloma. Best Pract of rare-earth radionuclides and other
magnitude of osteoblast involvement Res Clin Haematol 2007;20(4):625-635. bone-seekers in the evaluation of bone
lesions in patients with multiple
in order to determine whether the 5. Avet-Loiseau H, Attal M, Moreau P, myeloma or solitary plasmacytoma.
et al: Genetic abnormalities and survival
patient is a good candidate for this in multiple myeloma: The experience of
Radiology 1977;125(1):171-176.
treatment.2 the Intergroupe Francophone du 18. Orchard K, Barrington S, Buscombe J,
Myélome. Blood 2007;109(8):3489- Hilson A, Prentice HG, Mehta A:
3495. Fluoro-deoxyglucose positron emission
tomography imaging for the detection of
Summary 6. Rajkumar S, Fonseca R, Lacy M, et al: occult disease in multiple myeloma. Br J
Abnormal cytogenetics predict poor Haematol 2002;117(1):133-135.
survival after high-dose therapy and
Multiple myeloma is a primary ma- autologous blood cell transplantation in 19. Schirrmeister H, Bommer M, Buck AK,
lignancy of plasma cells that mani- multiple myeloma. Bone Marrow et al: Initial results in the assessment of
418 Journal of the American Academy of Orthopaedic Surgeons
Thomas J. Scharschmidt, MD, et al
multiple myeloma using 18F-FDG PET. 27. Barlogie B, Tricot GJ, van Rhee F, et al: bones: A proposed scoring system for
Eur J Nucl Med Mol Imaging 2002; Long-term outcome results of the first diagnosing impending pathologic
29(3):361-366. tandem autotransplant trial for multiple fractures. Clin Orthop Relat Res 1989;
myeloma. Br J Haematol 2006;135(2): (249):256-264.
20. Lütje S, de Rooy JW, Croockewit S, 158-164.
Koedam E, Oyen WJ, Raymakers RA: 36. Natarajan MV, Mohanlal P, Bose JC:
Role of radiography, MRI and FDG- 28. Bensinger WI, Maloney D, Storb R: The role of limb salvage surgery and
PET/CT in diagnosing, staging and Allogeneic hematopoietic cell custom mega prosthesis in multiple
therapeutical evaluation of patients with transplantation for multiple myeloma. myeloma. Acta Orthop Belg 2007;73(4):
Semin Hematol 2001;38(3):243-249. 462-467.
multiple myeloma. Ann Hematol 2009;
88(12):1161-1168. 37. Kivioja AH, Karaharju EO, Elomaa I,
29. Einsele H, Schäfer HJ, Hebart H, et al:
Follow-up of patients with progressive Böhling TO: Surgical treatment of
21. Mulligan ME, Badros AZ: PET/CT and
multiple myeloma undergoing allografts myeloma of bone. Eur J Cancer 1992;
MR imaging in myeloma. Skeletal 28A(11):1865-1869.
Radiol 2007;36(1):5-16. after reduced-intensity conditioning. Br J
Haematol 2003;121(3):411-418. 38. Cotten A, Dewatre F, Cortet B, et al:
22. Schirrmeister H, Buck AK, Bergmann L, Percutaneous vertebroplasty for
30. Kumar SK, Therneau TM, Gertz MA,
Reske SN, Bommer M: Positron emission osteolytic metastases and myeloma:
et al: Clinical course of patients with
tomography (PET) for staging of solitary Effects of the percentage of lesion filling
relapsed multiple myeloma. Mayo Clin
plasmacytoma. Cancer Biother and the leakage of methyl methacrylate
Proc 2004;79(7):867-874.
Radiopharm 2003;18(5):841-845. at clinical follow-up. Radiology 1996;
31. Rougraff BT, Kneisl JS, Simon MA: 200(2):525-530.
23. Dimopoulos MA, Moulopoulos LA, Skeletal metastases of unknown origin: A
Datseris I, et al: Imaging of myeloma prospective study of a diagnostic 39. Dürr HR, Wegener B, Krödel A, Müller
bone disease: Implications for staging, strategy. J Bone Joint Surg Am 1993; PE, Jansson V, Refior HJ: Multiple
prognosis and follow-up. Acta Oncol 75(9):1276-1281. myeloma: Surgery of the spine. Retro-
2000;39(7):823-827. spective analysis of 27 patients. Spine
32. Stanley A, Young A: Primary prevention (Phila Pa 1976) 2002;27(3):320-326.
24. Lecouvet FE, Dechambre S, Malghem J, of venous thromboembolism in medical
Ferrant A, Vande Berg BC, Maldague B: and surgical oncology patients. Br J 40. Yeh HS, Berenson JR: Treatment for
Bone marrow transplantation in patients Cancer 2010;102(suppl 1):S10-S16. myeloma bone disease. Clin Cancer Res
with multiple myeloma: Prognostic 2006;12(20 pt 2):6279S-6284S.
significance of MR imaging. AJR Am J 33. Proceedings of the seventh ACCP
Roentgenol 2001;176(1):91-96. conference on antithrombotic and 41. Holland J, Trenkner DA, Wasserman
thrombolytic therapy: Evidence-based TH, Fineberg B: Plasmacytoma:
25. Bladé J, Rosiñol L: Smoldering multiple guidelines. Chest 2004;126(3 suppl): Treatment results and conversion to
myeloma and monoclonal gammopathy 172S-696S. myeloma. Cancer 1992;69(6):1513-
of undetermined significance. Curr Treat 1517.
Options Oncol 2006;7(3):237-245. 34. Frassica FJ, Frassica DA: Evaluation and
treatment of metastases to the humerus. 42. Adamietz IA, Schöber C, Schulte RW,
26. Barlogie B, Tricot G, Anaissie E, et al: Clin Orthop Relat Res 2003;(415 suppl): Peest D, Renner K: Palliative
Thalidomide and hematopoietic-cell S212-S218. radiotherapy in plasma cell myeloma.
transplantation for multiple myeloma. N Radiother Oncol 1991;20(2):111-116.
Engl J Med 2006;354(10):1021-1030. 35. Mirels H: Metastatic disease in long
July 2011, Vol 19, No 7 419
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Design Thinking What It Is Owen Korea05Document17 pagesDesign Thinking What It Is Owen Korea05DanijelBaraNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Common Mistakes in Legal EnglishDocument4 pagesCommon Mistakes in Legal Englishfreshbreeze_2006No ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- RelativeResourceManager PDFDocument113 pagesRelativeResourceManager PDFMuhammad Irfan SalahuddinNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Đề Thi và Đáp ÁnDocument19 pagesĐề Thi và Đáp ÁnTruong Quoc TaiNo ratings yet
- Patient Risk for Self-Directed ViolenceDocument2 pagesPatient Risk for Self-Directed ViolenceGrape JuiceNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Galatians Part 5Document3 pagesGalatians Part 5nullvoice84No ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Guide 2017Document48 pagesGuide 2017Kleberson MeirelesNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Radiohead - The King of LimbsDocument2 pagesRadiohead - The King of LimbsOsmar LaraNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- SHDP TizonDocument29 pagesSHDP TizonRonnel Alegria RamadaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Testicular Self ExamDocument3 pagesTesticular Self ExamChristine JoyNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Sources of Strength For Mental Wellness by Sheryl Boswell, Youth Mental Health Canada (YMHC)Document11 pagesSources of Strength For Mental Wellness by Sheryl Boswell, Youth Mental Health Canada (YMHC)Youth Mental Health CanadaNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Literary Terms: Literatura/litteratura (Derived Itself From Littera: Letter or Handwriting)Document2 pagesLiterary Terms: Literatura/litteratura (Derived Itself From Littera: Letter or Handwriting)Berr WalidNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Target Mature Men with Luxury Watch MarketingDocument13 pagesTarget Mature Men with Luxury Watch MarketingAndriDwisondiNo ratings yet
- Ogham Gematria - Drawing Sephiroth6Document4 pagesOgham Gematria - Drawing Sephiroth6Simon StacheNo ratings yet
- Steps in Formatting Windows 7Document2 pagesSteps in Formatting Windows 7Marc RiomalosNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Assignment AnuDocument11 pagesAssignment AnuanushadaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Section 1: The Physical Self: Stages of Life SpanDocument4 pagesSection 1: The Physical Self: Stages of Life SpanMayo Nic3No ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Beyond The Wall - The Village Hero Character PlaybookDocument4 pagesBeyond The Wall - The Village Hero Character Playbookmagic_fyodorNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Transformations Women Gender and Psychology 3rd Edition Crawford Test BankDocument17 pagesTransformations Women Gender and Psychology 3rd Edition Crawford Test BankFrankDiazagsyr100% (12)
- 07Document30 pages07David MontoyaNo ratings yet
- Patient Medication ProfileDocument4 pagesPatient Medication ProfileLaura HernandezNo ratings yet
- Cryosurgery and ElectrosurgeryDocument51 pagesCryosurgery and ElectrosurgeryVeerabhadra RadhakrishnaNo ratings yet
- Proposal On The Goals For ChangeDocument5 pagesProposal On The Goals For ChangeMelody MhedzyNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Botanical Survey of IndiaDocument7 pagesBotanical Survey of IndiaParamjit Singh100% (2)
- CMRIT R18 Syllabus ME PDFDocument142 pagesCMRIT R18 Syllabus ME PDFMaddipudi RamakrishnaNo ratings yet
- Tao of Forgotten Food Diet - Taoist Herbology 2Document29 pagesTao of Forgotten Food Diet - Taoist Herbology 2ZioAngelNo ratings yet
- Jurnal-Ayu Santika NovinDocument10 pagesJurnal-Ayu Santika NovinSitti Hajar ONo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Case Study EntDocument22 pagesCase Study Entnurul syafiqah yahyaNo ratings yet
- TLE W3 EdwinlucinaDocument25 pagesTLE W3 Edwinlucinarhodora d. tamayoNo ratings yet
- TFN RVWDocument145 pagesTFN RVWmftaganasNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)