You might also like
- Laparoscopy AbscesoDocument7 pagesLaparoscopy AbscesoMedardo ApoloNo ratings yet
- American Dictations GastroDocument15 pagesAmerican Dictations GastroSaru BashaNo ratings yet
- Appendicitis SampleDocument15 pagesAppendicitis SampleChiqui Lao DumanhugNo ratings yet
- Successful Management of Giant Hydrocolpos in A LiDocument3 pagesSuccessful Management of Giant Hydrocolpos in A LiVictor FernandoNo ratings yet
- CP Yamat FinishDocument6 pagesCP Yamat FinishShiela GuiquingNo ratings yet
- Surgical ExamDocument302 pagesSurgical ExamHossam SabriNo ratings yet
- Acute Colonic Pseudo-Obstruction in Sickle Cell Disease: A Case ReportDocument4 pagesAcute Colonic Pseudo-Obstruction in Sickle Cell Disease: A Case ReportIJAR JOURNALNo ratings yet
- A Gigantic Ovarian Cyst A Case StudyDocument5 pagesA Gigantic Ovarian Cyst A Case Studyshaimaanassr25No ratings yet
- Cinical Scenario CholelithiasisDocument2 pagesCinical Scenario CholelithiasisSarine GonzalezNo ratings yet
- Chronic Gastric Dilatation With Gastric Fundus PerforationDocument4 pagesChronic Gastric Dilatation With Gastric Fundus Perforationvideo kedokteranNo ratings yet
- Appendicitis: " When The Bread Makes You Breathless ": Hendro Wartatmo Dept. of SurgeryDocument21 pagesAppendicitis: " When The Bread Makes You Breathless ": Hendro Wartatmo Dept. of SurgeryviviasriNo ratings yet
- Ectopic Abdominal Pregnancies: About 2 CasesDocument10 pagesEctopic Abdominal Pregnancies: About 2 CasesIJAR JOURNALNo ratings yet
- Gi 1Document3 pagesGi 1Syifa' FauziyahNo ratings yet
- 12b Clinical Update Example 2018Document9 pages12b Clinical Update Example 2018Ana BienneNo ratings yet
- J Epsc 2015 05 012Document4 pagesJ Epsc 2015 05 012Hanung PujanggaNo ratings yet
- Task of Plenary Discussion of Urinary System Block: Time Schedule: Thursday March 14, 2013 13.00-15.30 PMDocument3 pagesTask of Plenary Discussion of Urinary System Block: Time Schedule: Thursday March 14, 2013 13.00-15.30 PMabinadivegaNo ratings yet
- A Case Series of Candy Cane Limb Syndrome After Laparoscopic Roux-en-Y Gastric BypassDocument3 pagesA Case Series of Candy Cane Limb Syndrome After Laparoscopic Roux-en-Y Gastric BypassSavulescu OvidiuNo ratings yet
- Gastroenterology Cases PracticeDocument19 pagesGastroenterology Cases PracticeIbtissame BadadNo ratings yet
- Presentasi Mahasiswa Case 4 Blok Gis Semester 6 Tahun 2022Document52 pagesPresentasi Mahasiswa Case 4 Blok Gis Semester 6 Tahun 2022Tutde SedanaNo ratings yet
- Tubular Ileal Duplication Causing Small Bowel Obstruction in A ChildDocument5 pagesTubular Ileal Duplication Causing Small Bowel Obstruction in A ChildDiego Leonardo Herrera OjedaNo ratings yet
- Ms AJCRS 99757Document6 pagesMs AJCRS 99757Cesar DominguezNo ratings yet
- Article 1615981002 PDFDocument3 pagesArticle 1615981002 PDFMaria Lyn Ocariza ArandiaNo ratings yet
- Acute Surgical Abdomen: Unexpected Medical CauseDocument6 pagesAcute Surgical Abdomen: Unexpected Medical CauseIJAR JOURNALNo ratings yet
- Corpus Alienum in Rectosigmoid A Case ReportDocument4 pagesCorpus Alienum in Rectosigmoid A Case Reportlina ukagoNo ratings yet
- Acute Gastric Dilatation in ChildrenDocument6 pagesAcute Gastric Dilatation in ChildrenAkbar TabletNo ratings yet
- PDFDocument28 pagesPDFFauziyah ZiyahNo ratings yet
- Iatrogenic Injury To The Common Bile Duct: Case ReportDocument3 pagesIatrogenic Injury To The Common Bile Duct: Case ReportGianfranco MuntoniNo ratings yet
- Spontaneous Rupture of The Urinary Bladder A Case ReportDocument4 pagesSpontaneous Rupture of The Urinary Bladder A Case ReportAthenaeum Scientific PublishersNo ratings yet
- Myomectomy and Emergency Lap.Document19 pagesMyomectomy and Emergency Lap.SirAdjeteyNo ratings yet
- CasesDocument5 pagesCasesperiamaegan1No ratings yet
- C1 Atypical AppendicitisDocument1 pageC1 Atypical AppendicitisgeorgedejeuNo ratings yet
- SSIIP Case Studies Nov 2013Document32 pagesSSIIP Case Studies Nov 2013Anirban PaulNo ratings yet
- Essential Surgery (Textbook) - Review KROK-2 Type TestsDocument72 pagesEssential Surgery (Textbook) - Review KROK-2 Type Testsreihaneh mansouriNo ratings yet
- Post-cholecystectomy Bile Duct InjuryFrom EverandPost-cholecystectomy Bile Duct InjuryVinay K. KapoorNo ratings yet
- Vasquez - RLE A3 - PCCR (OSMUN Ward)Document16 pagesVasquez - RLE A3 - PCCR (OSMUN Ward)Mari Sheanne M. Vasquez100% (1)
- Case Report: The Combination of Gastroschisis, Jejunal Atresia, and Colonic Atresia in A NewbornDocument5 pagesCase Report: The Combination of Gastroschisis, Jejunal Atresia, and Colonic Atresia in A NewbornAnonymous PmfX227No ratings yet
- Oral Conception. Impregnation Via The Proximal Gastrointestinal Tract in A Patient With An Aplastic Distal Vagina. Case ReportDocument2 pagesOral Conception. Impregnation Via The Proximal Gastrointestinal Tract in A Patient With An Aplastic Distal Vagina. Case ReportwhochismoNo ratings yet
- Jurnal Diverticulum MeckelDocument18 pagesJurnal Diverticulum MeckelAnissa Aulia AdjaniNo ratings yet
- Case Report Small Intestinal Diverticulosis: A Rare Cause of Intestinal Perforation RevisitedDocument6 pagesCase Report Small Intestinal Diverticulosis: A Rare Cause of Intestinal Perforation RevisitedYeudiel SuroNo ratings yet
- JR 1Document10 pagesJR 1Yuni Purnama SariNo ratings yet
- Ojsadmin, 1032Document4 pagesOjsadmin, 1032Jade CentinoNo ratings yet
- An Antenatal Appearance of Megacystis-Microcolon-Intestinal Hypoperistalsis SyndromeDocument8 pagesAn Antenatal Appearance of Megacystis-Microcolon-Intestinal Hypoperistalsis SyndromeserubimNo ratings yet
- AppendicitisDocument14 pagesAppendicitisMary Joy BunuanNo ratings yet
- Case Protocol OB - H MOLEDocument3 pagesCase Protocol OB - H MOLEKim Adarem Joy ManimtimNo ratings yet
- Annsurg01101 0056Document4 pagesAnnsurg01101 0056Wendy LucasNo ratings yet
- Cholecystitis - Discharge SummaryDocument1 pageCholecystitis - Discharge SummaryIndranil SinhaNo ratings yet
- Diificult AirwayDocument13 pagesDiificult AirwayBhi-An BatobalonosNo ratings yet
- Adult Intussussception Int J Student Res 2012Document3 pagesAdult Intussussception Int J Student Res 2012Juan De Dios Diaz-RosalesNo ratings yet
- Duodenal Web at Bizarre LocationDocument22 pagesDuodenal Web at Bizarre LocationRAGHU NATH KARMAKERNo ratings yet
- Imcrj 11 113Document4 pagesImcrj 11 113fauziyatun nNo ratings yet
- Amj 23 2 235 240Document7 pagesAmj 23 2 235 240Czar Alexis FernandezNo ratings yet
- Appendicitis: San Roque Extension, Roxas City, Capiz 5800Document10 pagesAppendicitis: San Roque Extension, Roxas City, Capiz 5800GUEZIL JOY DELFINNo ratings yet
- Mortality and Morbidity Meeting PannirselvamDocument1 pageMortality and Morbidity Meeting PannirselvamMohammed SaleetNo ratings yet
- Management Dilemma in Case of Abdominal Pregnancy: A Case ReportDocument5 pagesManagement Dilemma in Case of Abdominal Pregnancy: A Case ReportDivika ShilvanaNo ratings yet
- Case Study - Pediatric HirshsprungDocument7 pagesCase Study - Pediatric Hirshsprungtruevine_ministryNo ratings yet
- Bariatric SurgeryDocument4 pagesBariatric SurgeryCla AlsterNo ratings yet
- Ectopic Pregnancy in Uncommon Implantation Sites: The Egyptian Journal of Radiology and Nuclear MedicineDocument10 pagesEctopic Pregnancy in Uncommon Implantation Sites: The Egyptian Journal of Radiology and Nuclear MedicinerezachandraNo ratings yet
- Case 5.Document3 pagesCase 5.rodeee789No ratings yet
- Colitis: A Practical Approach to Colon and Ileum Biopsy InterpretationFrom EverandColitis: A Practical Approach to Colon and Ileum Biopsy InterpretationAnne Jouret-MourinNo ratings yet
- Is 8Document4 pagesIs 8intan juitaNo ratings yet
- Is 2Document10 pagesIs 2intan juitaNo ratings yet
- Sisra JurnalDocument34 pagesSisra Jurnalintan juitaNo ratings yet
- Fingerhold Practice For Managing Emotions & StressDocument3 pagesFingerhold Practice For Managing Emotions & Stressintan juitaNo ratings yet
- Nurses' Roles in Health Promotion Practice: An Integrative ReviewDocument12 pagesNurses' Roles in Health Promotion Practice: An Integrative Reviewintan juitaNo ratings yet
- Is 9Document9 pagesIs 9intan juitaNo ratings yet
- Is C PDFDocument22 pagesIs C PDFintan juitaNo ratings yet
- The Future Role of Community Health Centers in ADocument15 pagesThe Future Role of Community Health Centers in Aintan juitaNo ratings yet
- Ijims 2015 117Document13 pagesIjims 2015 117intan juitaNo ratings yet
- Combined Double-Needle Flanged-Haptic Intrascleral Fixation of An Intraocular Lens and Descemet-Stripping Endothelial KeratoplastyDocument7 pagesCombined Double-Needle Flanged-Haptic Intrascleral Fixation of An Intraocular Lens and Descemet-Stripping Endothelial Keratoplastyintan juitaNo ratings yet
- Nursing Practice Review Ophthalmology: in This Article..Document7 pagesNursing Practice Review Ophthalmology: in This Article..intan juitaNo ratings yet
- Nurses Role in The Early Detection of CataractsDocument8 pagesNurses Role in The Early Detection of Cataractsintan juitaNo ratings yet
- Kuesioner Keluarga SejahteraDocument4 pagesKuesioner Keluarga Sejahteraintan juitaNo ratings yet
- Nursing Experience of 850 Cases On Centralized Cataract Surgery in CDPF Eyesight Recovery ProjectDocument4 pagesNursing Experience of 850 Cases On Centralized Cataract Surgery in CDPF Eyesight Recovery Projectintan juitaNo ratings yet
- Effectiveness of Orange Peelings As Insect Repellent: Mark Anthony Paul Borabo Jonard Estrallado Raff QuillosDocument4 pagesEffectiveness of Orange Peelings As Insect Repellent: Mark Anthony Paul Borabo Jonard Estrallado Raff QuillosAoki kazeNo ratings yet
- Yoana Cardenas: InternshipDocument2 pagesYoana Cardenas: Internshipapi-395953402No ratings yet
- Medical Declaration Form - Less Than 50 - EnglishDocument1 pageMedical Declaration Form - Less Than 50 - EnglishMohammed GeoffreyNo ratings yet
- Anaphylaxis: Learning ObjectivesDocument4 pagesAnaphylaxis: Learning Objectivesmohamed fahmyNo ratings yet
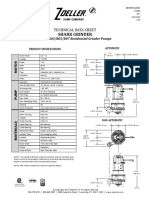
- Ficha Tecnica E803Document2 pagesFicha Tecnica E803Zenen AlarconNo ratings yet
- Edu Institutions in ErodeDocument4 pagesEdu Institutions in ErodeArvindSelvarajNo ratings yet
- RegistrationDocument130 pagesRegistrationJoanne AquinoNo ratings yet
- Clinical ResumeDocument6 pagesClinical Resumeapi-284041802No ratings yet
- PTM-TechRep-Hardness Measurement Cig CigFiltersDocument9 pagesPTM-TechRep-Hardness Measurement Cig CigFiltersRyan ChristiawanNo ratings yet
- (09032021) Press Release For Resumption of Selected Sports For NSG 2021 - MOEDocument2 pages(09032021) Press Release For Resumption of Selected Sports For NSG 2021 - MOEthesuperprogamer2 gamerNo ratings yet
- OPD and OT Days of Doctors of Clinical Department of Guru Gobind Singh Medical HospitalDocument4 pagesOPD and OT Days of Doctors of Clinical Department of Guru Gobind Singh Medical HospitalBohar singh Brar BrarNo ratings yet
- Cruz Marissa Resume CsusbDocument3 pagesCruz Marissa Resume Csusbapi-341233003No ratings yet
- Sickle Cell AnaemiaDocument8 pagesSickle Cell AnaemiaBhargav DesaiNo ratings yet
- Biflavones From Ginkgo Biloba As Inhibitors of Human ThrombinDocument10 pagesBiflavones From Ginkgo Biloba As Inhibitors of Human ThrombinmrsilNo ratings yet
- LSDE July 30 Tuesday 2013Document8 pagesLSDE July 30 Tuesday 2013LeyteSamar DailyExpressNo ratings yet
- Part InequalyDocument30 pagesPart Inequalycoga81No ratings yet
- ACCU20 (Encrypted)Document35 pagesACCU20 (Encrypted)kakiteNo ratings yet
- Industrial Pharmacy Lab ManualDocument46 pagesIndustrial Pharmacy Lab ManualDr. Anil LandgeNo ratings yet
- YANG SHENG 2011 October B PDFDocument70 pagesYANG SHENG 2011 October B PDFSasa PuiuNo ratings yet
- Literature Review On OgiDocument7 pagesLiterature Review On Ogiafdtaeczo100% (1)
- Enteral Nutrition (Gastrojejunotomy)Document30 pagesEnteral Nutrition (Gastrojejunotomy)Hairul IzlanNo ratings yet
- Kel 4 - BioethicsDocument22 pagesKel 4 - BioethicsLyana BerlyNo ratings yet
- Innovation at 3M - Group 3 - B2BDocument21 pagesInnovation at 3M - Group 3 - B2BRituraj BaruahNo ratings yet
- Ansi A10.42Document23 pagesAnsi A10.42pedro la rosa100% (1)
- Herppvc PDFDocument6 pagesHerppvc PDFDr.Chetana INo ratings yet
- Vaccine Guide - Randall NeustaedterDocument6 pagesVaccine Guide - Randall NeustaedterttreksNo ratings yet
- The Role of The Nurse in Health Promotion PDFDocument1 pageThe Role of The Nurse in Health Promotion PDFCie Ladd0% (1)
- Gymnemic AcidDocument9 pagesGymnemic AcidarumpratiwiNo ratings yet
- N222 Lecture Notes Sp13Document198 pagesN222 Lecture Notes Sp13Jacinth Florido FedelinNo ratings yet
- A Rapid Filtration Method For Harvesting Cell Cultture Grown in Cellbag Bio ReactorsDocument4 pagesA Rapid Filtration Method For Harvesting Cell Cultture Grown in Cellbag Bio ReactorsfreefreederNo ratings yet