You might also like
- Instructors Manual Management Control SyDocument40 pagesInstructors Manual Management Control SySatria AstaNo ratings yet
- Case Study - Family Care Specialists Medical Group, Inc.Document7 pagesCase Study - Family Care Specialists Medical Group, Inc.Nicholas AlexanderNo ratings yet
- DS-RTCD905 H6W4Document2 pagesDS-RTCD905 H6W4david fonsecaNo ratings yet
- Measuring and Controlling Assets at Aloha ProductsDocument2 pagesMeasuring and Controlling Assets at Aloha ProductsDenisse MontesNo ratings yet
- Global InvestorsDocument36 pagesGlobal InvestorsIda Agustini50% (2)
- Hitungan Kuis 7 Bunyan - Lumber - CaseDocument15 pagesHitungan Kuis 7 Bunyan - Lumber - Caserica100% (1)
- J&L Railroad Hedging StrategiesDocument2 pagesJ&L Railroad Hedging StrategiesAde AdeNo ratings yet
- Desktop Solution IncDocument6 pagesDesktop Solution IncAmira Nur Afiqah Agus Salim0% (1)
- Jawaban Case B TexasDocument7 pagesJawaban Case B TexasGilangRamadhanNo ratings yet
- Tradeoff Relevance and Reliability Cash Flow EstimatesDocument5 pagesTradeoff Relevance and Reliability Cash Flow EstimatesKrithika NaiduNo ratings yet
- Ethylene Yield From Pyrolysis Cracking in Olefin PDocument6 pagesEthylene Yield From Pyrolysis Cracking in Olefin PALL2WINNo ratings yet
- Confined Space: Hole Watch TrainingDocument36 pagesConfined Space: Hole Watch TrainingMalik JunaidNo ratings yet
- Positive Theory of Accounting Policy and DisclosureDocument6 pagesPositive Theory of Accounting Policy and DisclosureMirnah AmirNo ratings yet
- P V: The Case Will Be Analyzed From The Standpoint of TheDocument3 pagesP V: The Case Will Be Analyzed From The Standpoint of ThecesarvirataNo ratings yet
- 7 1 Haengbok Bancorp RZDocument4 pages7 1 Haengbok Bancorp RZAnatasyaOktavianiHandriatiTataNo ratings yet
- Accounting Measurement SystemDocument7 pagesAccounting Measurement SystemDionysius Ivan Hertanto100% (1)
- Exam Unit 1 Out and About 1º BachilleratoDocument5 pagesExam Unit 1 Out and About 1º Bachilleratolisikratis1980No ratings yet
- Chapter 3 Action, Personnel, and Cultural ControlsDocument15 pagesChapter 3 Action, Personnel, and Cultural ControlsAdrian ChrisceydiNo ratings yet
- 2017 Expert Packet Workshop V3 + ExerciseDocument268 pages2017 Expert Packet Workshop V3 + ExerciseJeya ChandranNo ratings yet
- Manajemen Laba (Earnings Management)Document35 pagesManajemen Laba (Earnings Management)ricky OkNo ratings yet
- Building Lean Supply ChainsDocument33 pagesBuilding Lean Supply ChainsJefri MustaphaNo ratings yet
- "A Study Consumer Satisfaction Towards Royal Enfield BikesDocument72 pages"A Study Consumer Satisfaction Towards Royal Enfield BikesKotresh Kp100% (1)
- T2-1 MS PDFDocument27 pagesT2-1 MS PDFManav NairNo ratings yet
- Hoffman Discount Drug IncDocument1 pageHoffman Discount Drug IncJacky DoanNo ratings yet
- PCL TVDocument4 pagesPCL TVEm MonteNo ratings yet
- Case Study - Kranworth Chair CorporationDocument3 pagesCase Study - Kranworth Chair CorporationMaruli Tua SianturiNo ratings yet
- Implementing Strategy with Performance Measurement SystemsDocument22 pagesImplementing Strategy with Performance Measurement SystemsAzaan Kaul100% (2)
- Premium for Good Corporate GovernanceDocument5 pagesPremium for Good Corporate GovernancelaloasisNo ratings yet
- Beams11 Ppt10 EDITDocument46 pagesBeams11 Ppt10 EDITAgoeng Susanto BrajewoNo ratings yet
- Johnson & Johnson’s sustainability reporting process (2010 report) and changes in 2019 reportDocument4 pagesJohnson & Johnson’s sustainability reporting process (2010 report) and changes in 2019 reportMaria fayyazNo ratings yet
- Contemporary Issues in Accounting: Solution ManualDocument20 pagesContemporary Issues in Accounting: Solution ManualKeiLiew0% (1)
- Jawaban GSLC 1Document2 pagesJawaban GSLC 1Soniea DianiNo ratings yet
- Case SPMDocument4 pagesCase SPMainiNo ratings yet
- A Critique of Conceptual Framework ProjectsDocument12 pagesA Critique of Conceptual Framework ProjectsJhoNo ratings yet
- Case 1-3 XEROX - Mardiyah Isma Hidayati - 1101002026Document4 pagesCase 1-3 XEROX - Mardiyah Isma Hidayati - 1101002026Mardiyah Isma HidayatiNo ratings yet
- Analyzing Returns and Effects of LeverageDocument4 pagesAnalyzing Returns and Effects of LeverageCiptawan CenNo ratings yet
- Mini Case STOCK VALUATIONDocument5 pagesMini Case STOCK VALUATIONRizky Khairunnisa0% (1)
- Emerson Electric Strategic Cost Management Case StudyDocument3 pagesEmerson Electric Strategic Cost Management Case StudyCahyo Priyatno0% (1)
- Ch7 Measuring and Controlling Assets EmployedDocument5 pagesCh7 Measuring and Controlling Assets EmployedKeren MilletNo ratings yet
- Waysideinnsincgroupm 110520054120 Phpapp02Document7 pagesWaysideinnsincgroupm 110520054120 Phpapp02raghunomix123No ratings yet
- CHAPTER 3 (Topic 4) - GODFREYDocument53 pagesCHAPTER 3 (Topic 4) - GODFREYAdobe Pro100% (1)
- HomeWork MCS-Nurul Sari (1101002048) - Case 5.1 5.4Document5 pagesHomeWork MCS-Nurul Sari (1101002048) - Case 5.1 5.4Nurul SariNo ratings yet
- Mini Case: Stock Valuation at Ragan Engines: Disusun OlehDocument6 pagesMini Case: Stock Valuation at Ragan Engines: Disusun OlehricaNo ratings yet
- Chapter One: Mcgraw-Hill/IrwinDocument17 pagesChapter One: Mcgraw-Hill/Irwinteraz2810No ratings yet
- Organizing and Controlling Profit CentersDocument3 pagesOrganizing and Controlling Profit CentersTiffany SmithNo ratings yet
- Rendell CompanyDocument3 pagesRendell CompanyTung Nguyen KhacNo ratings yet
- Comparing Planning and Control Systems of Texas Instruments and Hewlett-PackardDocument20 pagesComparing Planning and Control Systems of Texas Instruments and Hewlett-PackardNaveen SinghNo ratings yet
- Universiti Utara Malaysia Othman Yeop Abdullah Graduate School of Business (Oyagsb) A201 2020/2021Document2 pagesUniversiti Utara Malaysia Othman Yeop Abdullah Graduate School of Business (Oyagsb) A201 2020/2021fitriNo ratings yet
- Cup CorporationDocument17 pagesCup Corporationandri100% (1)
- Chapter 5 - Financial Management and Policies - SyllabusDocument7 pagesChapter 5 - Financial Management and Policies - SyllabusharithraaNo ratings yet
- TI vs HP management control systemsDocument3 pagesTI vs HP management control systemsMuhammad KamilNo ratings yet
- Post-retirement benefits practice exercises solutionsDocument4 pagesPost-retirement benefits practice exercises solutionsJulian Christopher Torcuator50% (2)
- ERP Helps Productivity at Northern Digital IncDocument10 pagesERP Helps Productivity at Northern Digital IncLihin100% (1)
- Jensen Corporation Is A Holding Company With Several DiversifiedDocument2 pagesJensen Corporation Is A Holding Company With Several DiversifiedAmit PandeyNo ratings yet
- SPM Case Tsinghua Tongfang Co. LTDDocument2 pagesSPM Case Tsinghua Tongfang Co. LTDNur Kumala Dewi100% (2)
- ACC 4291 Group Case Summary: Beifang Chuang Ye Vehicle GroupDocument10 pagesACC 4291 Group Case Summary: Beifang Chuang Ye Vehicle GroupUmar AzizNo ratings yet
- AFIN1Document6 pagesAFIN1Abs PangaderNo ratings yet
- Cvs Health Valuation Fin 4310 Semester ProjectDocument26 pagesCvs Health Valuation Fin 4310 Semester Projectapi-283720057No ratings yet
- Ada Pharmaceutical Company Produces Three Drugs Diomycin HomycDocument2 pagesAda Pharmaceutical Company Produces Three Drugs Diomycin HomycAmit PandeyNo ratings yet
- Teori AkunDocument12 pagesTeori AkunErditama GeryNo ratings yet
- New Jersey Insurance CompanyDocument13 pagesNew Jersey Insurance CompanyParth V. PurohitNo ratings yet
- Sharpe RatioDocument13 pagesSharpe RatioArimas FirasNo ratings yet
- Macroeconomic and Industry AnalysisDocument4 pagesMacroeconomic and Industry AnalysisFajar TaufiqNo ratings yet
- Lecture 2 - Answer Part 2Document6 pagesLecture 2 - Answer Part 2Thắng ThôngNo ratings yet
- Kok Banyak Anying Tugas eDocument7 pagesKok Banyak Anying Tugas eJim ChaNo ratings yet
- Cost of Education and Earning Potential For Non-Physician Anesthesia ProvidersDocument8 pagesCost of Education and Earning Potential For Non-Physician Anesthesia ProvidersIlvita MayasariNo ratings yet
- Uploading To DowloadDocument13 pagesUploading To DowloadTyler RuizNo ratings yet
- Microeconomic Analysis Physician - mw2Document9 pagesMicroeconomic Analysis Physician - mw2Megan W.No ratings yet
- Kas b2c 2022 AprilDocument1 pageKas b2c 2022 AprilainiNo ratings yet
- Resume SIA 2 Chapter 14Document7 pagesResume SIA 2 Chapter 14ainiNo ratings yet
- Case SPMDocument4 pagesCase SPMainiNo ratings yet
- Resume SIA 2 Chapter 14Document7 pagesResume SIA 2 Chapter 14ainiNo ratings yet
- How To Critique A Photograph - Facebook PDFDocument1 pageHow To Critique A Photograph - Facebook PDFpeterNo ratings yet
- Database AwsDocument15 pagesDatabase AwsHareesha N GNo ratings yet
- Master in Public Management: Application PacketDocument6 pagesMaster in Public Management: Application PacketMark GironNo ratings yet
- RRT LH: Gt'R:Ut (TLDocument75 pagesRRT LH: Gt'R:Ut (TLkl equipmentNo ratings yet
- Examining The Structural Relationships of Destination Image, Tourist Satisfaction PDFDocument13 pagesExamining The Structural Relationships of Destination Image, Tourist Satisfaction PDFAndreea JecuNo ratings yet
- Consumer Notebook Price List For September 2010Document4 pagesConsumer Notebook Price List For September 2010Anand AryaNo ratings yet
- Accounting For Non Specialists Australian 7th Edition Atrill Test BankDocument26 pagesAccounting For Non Specialists Australian 7th Edition Atrill Test BankJessicaMitchelleokj100% (49)
- Strategic Marketing Plan for British American TobaccoDocument31 pagesStrategic Marketing Plan for British American TobaccoAli Abbas50% (2)
- My Demo DemoDocument19 pagesMy Demo DemoAlex LopezNo ratings yet
- Slide Detail For SCADADocument20 pagesSlide Detail For SCADAhakimNo ratings yet
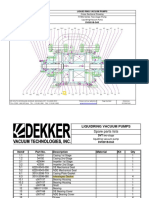
- Bomba de Vacio Part ListDocument2 pagesBomba de Vacio Part ListNayeli Zarate MNo ratings yet
- Boston Globe Article - Jonnie Williams & Frank O'DonnellDocument3 pagesBoston Globe Article - Jonnie Williams & Frank O'DonnellFuzzy PandaNo ratings yet
- HL-1060 User, Parts, and Service Manual 02Document6 pagesHL-1060 User, Parts, and Service Manual 02วรพงษ์ กอชัชวาลNo ratings yet
- Julia Henzler - Resume 2 27Document1 pageJulia Henzler - Resume 2 27api-491391730No ratings yet
- Method Overloading in JavaDocument6 pagesMethod Overloading in JavaPrerna GourNo ratings yet
- LogDocument15 pagesLogandrew_hm925635No ratings yet
- GRP 10 JV'sDocument43 pagesGRP 10 JV'sManas ChaturvediNo ratings yet
- 1 Catalyst FundamentalsDocument17 pages1 Catalyst FundamentalsSam AnuNo ratings yet
- ErgonomicsDocument15 pagesErgonomicsdtmNo ratings yet
- What Is Mean?: Extrapolation InterpolationDocument2 pagesWhat Is Mean?: Extrapolation InterpolationVinod SharmaNo ratings yet
- 10 - (Rahman) The Relationship Between Chest Tube Size and Clinical Outcome in Pleural InfectionDocument8 pages10 - (Rahman) The Relationship Between Chest Tube Size and Clinical Outcome in Pleural InfectionfaisaldanyaniNo ratings yet
- 6.1.2 The Solar SystemDocument4 pages6.1.2 The Solar System205 NursyazliyanaNo ratings yet