You might also like
- Physical Assessment Guide of Head-To-ToeDocument9 pagesPhysical Assessment Guide of Head-To-Toeneleh gray100% (2)
- Gastrointestinal Physical Exam Checklist 1Document1 pageGastrointestinal Physical Exam Checklist 1Assma Haytham Murad100% (2)
- H&P OutlineDocument5 pagesH&P Outlineginadaislu100% (1)
- 3 SOAP Presentation Template 5.19.16 PDFDocument1 page3 SOAP Presentation Template 5.19.16 PDFnems92No ratings yet
- NU 260-Pediatric Assessment FormDocument3 pagesNU 260-Pediatric Assessment FormMarie Holder67% (6)
- Physical Examination ChecklistDocument5 pagesPhysical Examination Checklistsamhie21No ratings yet
- Contraception Soap Note: Running HeadDocument7 pagesContraception Soap Note: Running HeadAnnah AnnNo ratings yet
- Uterine Fibroids Case StudyDocument38 pagesUterine Fibroids Case StudyFiona Cheryl Amsterdam80% (5)
- Care Plan Handbook TemplateDocument34 pagesCare Plan Handbook TemplateBreanna Hopkins100% (1)
- Case PresentationDocument30 pagesCase PresentationAmira HelayelNo ratings yet
- Pediatric 101 Vital SignsDocument2 pagesPediatric 101 Vital SignsAyeshah RosdahNo ratings yet
- History and Physical ExaminationDocument7 pagesHistory and Physical ExaminationKathleen Cedillo100% (1)
- Comprehensive H&PDocument2 pagesComprehensive H&PjwwisnerNo ratings yet
- General Rules of Abdomenal ExaminationDocument22 pagesGeneral Rules of Abdomenal ExaminationSamuel Sebastian SirapanjiNo ratings yet
- The Following List Illustrates The Content of A Complete Review of SystemsDocument1 pageThe Following List Illustrates The Content of A Complete Review of SystemsHazel CastorNo ratings yet
- Hospital Follow Up Progress Note MedicalTemplateDocument1 pageHospital Follow Up Progress Note MedicalTemplatee-MedTools100% (18)
- Bates Physical Examination RED NOTESDocument2 pagesBates Physical Examination RED NOTESAmanda Gomez100% (1)
- History & Physical Diagnostic#Document106 pagesHistory & Physical Diagnostic#Olsa Alshapira100% (1)
- Soap Note Handout 06Document24 pagesSoap Note Handout 06Charie Joyce Go100% (1)
- Health HistoryDocument19 pagesHealth HistoryAngelene Caliva100% (1)
- Focused AssessmentDocument5 pagesFocused AssessmentPiyali SahaNo ratings yet
- Conduct of Physical Examination: I. General SurveyDocument10 pagesConduct of Physical Examination: I. General SurveyWeng RamojalNo ratings yet
- History Taking and PEDocument30 pagesHistory Taking and PEMelissa Salayog100% (1)
- SOAP For Upper Respiratory Infection #4Document3 pagesSOAP For Upper Respiratory Infection #4carlos fernandezNo ratings yet
- ICU Rounding Template - v. WebsiteDocument2 pagesICU Rounding Template - v. Websitepattumkp0% (1)
- Bates Chapter 2 Flashcards - QuizletDocument6 pagesBates Chapter 2 Flashcards - Quizletaznknight323No ratings yet
- Review of SystemsDocument4 pagesReview of SystemsJason Kai Poth100% (1)
- SOAP Notes-WPS OfficeDocument11 pagesSOAP Notes-WPS OfficeNexi anessaNo ratings yet
- General History and Physical Examination FormDocument2 pagesGeneral History and Physical Examination FormQueen Hera100% (1)
- Diabetes SoapDocument1 pageDiabetes Soapmurex8125No ratings yet
- Typhon CasesDocument5 pagesTyphon Casesapi-483865455No ratings yet
- Surgery History and Physical ExaminationDocument3 pagesSurgery History and Physical ExaminationKarsten RohlfsNo ratings yet
- Nursing NoteDocument6 pagesNursing Noteshiller0% (1)
- Obgyn DocumentationDocument13 pagesObgyn DocumentationEli EidNo ratings yet
- Suggested Order For History and Physical Examination DocumentationDocument2 pagesSuggested Order For History and Physical Examination DocumentationNicole BrassingtonNo ratings yet
- Cardiovascular BigDocument37 pagesCardiovascular Bigfaiz nasirNo ratings yet
- Checklist For Physical Examination of KneeDocument13 pagesChecklist For Physical Examination of KneeGuruprasanth PazhamalaiNo ratings yet
- Pain Case - SOAP Note (2011)Document2 pagesPain Case - SOAP Note (2011)Alfie Lee100% (3)
- A Guide To Physical ExaminationDocument73 pagesA Guide To Physical ExaminationDessy AmaranthaNo ratings yet
- Physical Exam ChecklistDocument2 pagesPhysical Exam ChecklistRaisah Bint Abdullah100% (5)
- Physical Examination GuideDocument3 pagesPhysical Examination GuideKarl Jimenez Separa100% (2)
- Abdominal Trauma II PDFDocument6 pagesAbdominal Trauma II PDFJohn Christopher LucesNo ratings yet
- Physical Exam Final Written Exam Study Guide 2Document51 pagesPhysical Exam Final Written Exam Study Guide 2pelly3190100% (2)
- A. Subjective: 1. Progress NoteDocument3 pagesA. Subjective: 1. Progress NoteEvan100% (1)
- Soap NoteDocument2 pagesSoap NoteLlosa June50% (2)
- Guide To The Comprehensive Pediatric H and P Write Up PDFDocument16 pagesGuide To The Comprehensive Pediatric H and P Write Up PDFnanaNo ratings yet
- Peds Study GuideDocument73 pagesPeds Study GuideYvonne Huang100% (1)
- History and Physical SheetDocument4 pagesHistory and Physical Sheetjonnyahn100% (1)
- Soap 2 - PainDocument6 pagesSoap 2 - Painapi-482726932No ratings yet
- Soap TemplateDocument3 pagesSoap TemplaterohitNo ratings yet
- Physical Examination Health AssessmentDocument2 pagesPhysical Examination Health AssessmentRosa Willis0% (1)
- Diabetes and Complications: When Documenting Diabetes, It's Important To Note The FollowingDocument2 pagesDiabetes and Complications: When Documenting Diabetes, It's Important To Note The Followingmeikaizen100% (1)
- Guide in Reporting Complete Physical Examination (2013) - Source: Bates' Guide To Physical Examination.Document8 pagesGuide in Reporting Complete Physical Examination (2013) - Source: Bates' Guide To Physical Examination.Ernie G. Bautista II, RN, MD100% (6)
- Audit FormsDocument4 pagesAudit Formsapi-349641525No ratings yet
- MS3 Survival GuideDocument50 pagesMS3 Survival Guideprahul2588No ratings yet
- Megs History PhysicalDocument1 pageMegs History Physicalrmelendez001No ratings yet
- Spinal Head InjuryDocument2 pagesSpinal Head Injuryapi-238082157No ratings yet
- Older Adult - Soap 2 PDFDocument4 pagesOlder Adult - Soap 2 PDFSavanna EarleNo ratings yet
- HPI For History and Physical ExamDocument2 pagesHPI For History and Physical Examv-santNo ratings yet
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Laporan Hasil Pemeriksaan Laboratorium Mikrobiologi Klinik Departemen Mikrobiologi Fakultas Kedokteran Universitas IndonesiaDocument10 pagesLaporan Hasil Pemeriksaan Laboratorium Mikrobiologi Klinik Departemen Mikrobiologi Fakultas Kedokteran Universitas IndonesiaPrincella MonicaNo ratings yet
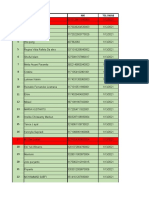
- No Lab No CM No Nik Nama Pasien Tanggal PCR NO Sampel Jenis Kelamin Tanggal Lahir Tanggal SwabDocument1 pageNo Lab No CM No Nik Nama Pasien Tanggal PCR NO Sampel Jenis Kelamin Tanggal Lahir Tanggal SwabPrincella MonicaNo ratings yet
- Draft Shift 2020Document10 pagesDraft Shift 2020Princella MonicaNo ratings yet
- Has13012021 Batch2Document6 pagesHas13012021 Batch2Princella MonicaNo ratings yet
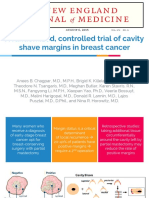
- RCT: Cavity Shave MarginDocument8 pagesRCT: Cavity Shave MarginPrincella MonicaNo ratings yet
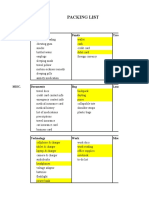
- Packing List: Destination Days Basics Travel Aids Funds Travel InfoDocument5 pagesPacking List: Destination Days Basics Travel Aids Funds Travel InfoPrincella MonicaNo ratings yet
- Dypsnea - RevisedDocument19 pagesDypsnea - RevisedPrincella MonicaNo ratings yet
- Diagnostic Value of Nystagmus: Spontaneous and Induced Ocular OscillationsDocument5 pagesDiagnostic Value of Nystagmus: Spontaneous and Induced Ocular OscillationsPrincella MonicaNo ratings yet
- Placenta Previa: Supervised By: Dr. Pim Gonta, SP - OGDocument24 pagesPlacenta Previa: Supervised By: Dr. Pim Gonta, SP - OGPrincella MonicaNo ratings yet
- 7th Edition NRP Update FinalDocument18 pages7th Edition NRP Update FinalPrincella MonicaNo ratings yet
- (Digestive System) : Khan G. S. Research Centre Khan G. S. Research CentreDocument7 pages(Digestive System) : Khan G. S. Research Centre Khan G. S. Research CentreGopal ShawNo ratings yet
- Rhesus IsoimmunisationDocument27 pagesRhesus IsoimmunisationMuwanga faizoNo ratings yet
- Friday Seminar 9-23Document28 pagesFriday Seminar 9-23api-609125382No ratings yet
- Efficacy and Safety of Bepirovirsen in Chronic Hepatitis B InfectionDocument12 pagesEfficacy and Safety of Bepirovirsen in Chronic Hepatitis B InfectionArif AlvaNo ratings yet
- Socratic Discussion 1 QuestionsDocument4 pagesSocratic Discussion 1 Questionsapi-296326751No ratings yet
- Sample of Job DescriptionsDocument48 pagesSample of Job DescriptionsLoresita Amoranto Rebong RNNo ratings yet
- TizanidineDocument2 pagesTizanidinebhawanisrNo ratings yet
- Berberine Ameliorates Hyperglycemia in Alloxan-Induced Diabetic C57BL/6 Mice Through Activation of Akt Signaling PathwayDocument8 pagesBerberine Ameliorates Hyperglycemia in Alloxan-Induced Diabetic C57BL/6 Mice Through Activation of Akt Signaling PathwaySunny Side Up SunNo ratings yet
- Global Regenerative Group Becomes Global Distributor For Pharmaceutical Wholesaler Prosupplier GMBH Representing Their CureOs® Synthetic BONE GRAFTDocument3 pagesGlobal Regenerative Group Becomes Global Distributor For Pharmaceutical Wholesaler Prosupplier GMBH Representing Their CureOs® Synthetic BONE GRAFTPR.comNo ratings yet
- Management of SnakebiteDocument67 pagesManagement of SnakebiteHui TingNo ratings yet
- First AidDocument37 pagesFirst AidPearl Delay100% (1)
- JUH Residency Entrance Exam 2021Document5 pagesJUH Residency Entrance Exam 2021leenamro1999No ratings yet
- Dasatinib Monograph 1mar2017Document8 pagesDasatinib Monograph 1mar2017Fandi HarmikiNo ratings yet
- Occlusion in FPDDocument108 pagesOcclusion in FPDVishal ReddyNo ratings yet
- Suppositories Dosage Forms by ShironDocument2 pagesSuppositories Dosage Forms by ShironShiron PathiranaNo ratings yet
- Cancer Prevention and ControlDocument3 pagesCancer Prevention and ControlMarwin OditaNo ratings yet
- Open Letter To The CMOs of England, Wales, Scotland and Northern IrelandDocument4 pagesOpen Letter To The CMOs of England, Wales, Scotland and Northern IrelandThe Guardian100% (11)
- Retinal Detachment: Case Report Operating RoomDocument30 pagesRetinal Detachment: Case Report Operating RoomCarlo Joseph Intal LlacerNo ratings yet
- HDL-C Direct FS : Order Information ReagentsDocument3 pagesHDL-C Direct FS : Order Information ReagentsmnemonicsNo ratings yet
- Sindrom AlagileDocument8 pagesSindrom AlagilewenyinriantoNo ratings yet
- Llista de Microrganismos Dano de Barreira MucosaDocument19 pagesLlista de Microrganismos Dano de Barreira MucosaThereza LimaNo ratings yet
- Concepts in Public He Alth: A Case Study of Protein Energy Malnutrition (PEM)Document21 pagesConcepts in Public He Alth: A Case Study of Protein Energy Malnutrition (PEM)Aswin AshNo ratings yet
- National High Blood Pressure Education Program Working Group Rep 1990Document22 pagesNational High Blood Pressure Education Program Working Group Rep 1990carlosarmijoNo ratings yet
- The Term Aplastic Anemia Indicates: Pancytopenia in The PresenceDocument34 pagesThe Term Aplastic Anemia Indicates: Pancytopenia in The PresenceKhadar mohamedNo ratings yet
- Physical Fitness NotesDocument4 pagesPhysical Fitness NotesAmy Chang0% (1)
- Leaflet - Milk FermentationDocument3 pagesLeaflet - Milk FermentationNoor SultanNo ratings yet
- OCSA Clinical Student Health FormDocument2 pagesOCSA Clinical Student Health Formimdaking123No ratings yet
- BibliographyDocument2 pagesBibliographyMajkel Benche CustodioNo ratings yet
- Soal Try Out II SBMPTN 2018 Paket 320Document3 pagesSoal Try Out II SBMPTN 2018 Paket 320Siappudan Ni DainangNo ratings yet