Professional Documents
Culture Documents
Management of Distal Clavicle Fractures
Management of Distal Clavicle Fractures
Uploaded by
JayCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Management of Distal Clavicle Fractures
Management of Distal Clavicle Fractures
Uploaded by
JayCopyright:
Available Formats
Review Article
Management of Distal Clavicle
Fractures
Abstract
Rahul Banerjee, MD Most clavicle fractures heal without difficulty. However, radiographic
Brian Waterman, MD nonunion after distal clavicle fracture has been reported in 10% to
44% of patients. Type II distal clavicle fractures, which involve
Jeff Padalecki, MD
displacement, are associated with the highest incidence of
William Robertson, MD nonunion. Several studies have questioned the clinical relevance of
distal clavicle nonunion, however. Nonsurgical and surgical
management provide similar results. The decision whether to
operate may be influenced by the amount of fracture displacement
and the individual demands of the patient. Surgical options to
achieve bony union include transacromial wire fixation, a modified
Weaver-Dunn procedure, use of a tension band, screw fixation,
plating, and arthroscopy. Each technique has advantages and
disadvantages; insufficient evidence exists to demonstrate that any
one technique consistently provides the best results.
From the Department of
Orthopaedic Surgery, University of
Texas Southwestern Medical Center,
Dallas, TX (Dr. Banerjee,
F ractures of the distal clavicle ac-
count for approximately 10% to
30% of all clavicle fractures.1 Man-
not only which distal clavicle frac-
tures require surgical fixation but
also which fixation method is best.
Dr. Padalecki, and Dr. Robertson), agement of distal clavicle fractures is
and the Department of Orthopaedic
Surgery and Rehabilitation, Texas often challenging because of the dif-
Tech University Health Sciences ficulty in distinguishing subtle varia- Anatomy and
Center, El Paso, TX (Dr. Waterman). tions in the fracture pattern that may Biomechanics
Dr. Banerjee or an immediate family indicate fracture instability. Stable The clavicle serves as a strut connect-
member has received research or fracture patterns generally heal un-
institutional support from Synthes,
ing the upper extremity to the appen-
eventfully with nonsurgical manage- dicular skeleton. Fluid scapulotho-
Smith & Nephew, Medtronic, and
Stryker, and serves as a board ment, but unstable fracture patterns racic motion is dependent on a stable
member, owner, officer, or are often associated with longer time relationship between the distal clavi-
committee member of the American to union and notable nonunion rates.
Academy of Orthopaedic Surgeons.
cle and the scapula. This stability is
Dr. Robertson serves as a paid Because of concern that nonsurgi- provided by the acromioclavicular
consultant to ConMed Linvatec. cal management may result in non- (AC) joint capsule, AC ligaments,
Neither of the following authors nor union, primary surgical management and coracoclavicular (CC) ligaments.
any immediate family member has
received anything of value from or
has been recommended for certain The AC ligaments span the AC
owns stock in a commercial distal clavicle fracture patterns.2-6 joint, attaching to both the medial
company or institution related However, these nonunions are often aspect of the acromion and the distal
directly or indirectly to the subject of asymptomatic, and their clinical rele- extent of the clavicle and reinforcing
this article: Dr. Waterman and
Dr. Padalecki. vance has been questioned.1,7 The use the AC joint capsule. These liga-
of nonsurgical management is bol- ments serve as an important stabi-
J Am Acad Orthop Surg 2011;19:
392-401
stered by the various complications lizer to horizontal (AP) motion at the
that have historically been reported AC joint.8 This capsuloligamentous
Copyright 2011 by the American
following surgical fixation. As a re- complex attaches to the distal aspect
Academy of Orthopaedic Surgeons.
sult, there is uncertainty regarding of the clavicle approximately 6 mm
392 Journal of the American Academy of Orthopaedic Surgeons
Rahul Banerjee, MD, et al
medial to the AC joint.9 Figure 1
The CC ligaments (ie, trapezoid,
conoid) originate at the base of the
coracoid process of the scapula and
insert on the undersurface of the dis-
tal clavicle. The trapezoid is the
more lateral of the two ligaments
and attaches to the distal clavicle
approximately 2 cm from the AC
joint.9 The conoid ligament, which is
located more medially, attaches to
the clavicle approximately 4 cm from
the AC joint. These ligaments play a
pivotal role in preventing superior
displacement of the distal clavicle in
relation to the acromion. The normal
distance between the coracoid pro-
cess and the undersurface of the clav-
icle (ie, CC interspace) is 1.1 to 1.3
cm.10
The clavicle also serves as an im-
portant origin and site of insertion
for several muscles involved in mo-
tion of the shoulder and the cervical
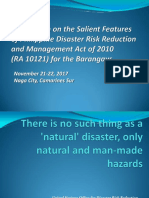
spine, including the sternocleidomas- Illustration of the Neer classification of distal clavicle fractures. Type I fracture
occurs distal to the coracoclavicular (CC) ligaments (ie, trapezoid, conoid)
toid, anterior deltoid, and trapezius. and involves minimal fracture displacement. The acromioclavicular (AC) joint
Depending on the fracture pattern, remains intact. Type IIA fracture occurs medial to the conoid ligament. Type
these muscles can create deforming IIB fracture occurs between the CC ligaments and includes disruption of the
forces. Neer4 described four deform- conoid ligament. The trapezoid ligament remains intact. Type III fracture
occurs distal to the CC ligaments and extends into the AC joint. Type IV
ing forces: weight of the arm; pull of fracture occurs in pediatric patients. The physis and epiphysis remain
the pectoralis major, pectoralis mi- adjacent to the AC joint, but there is displacement at the junction of the
nor, and latissimus dorsi muscles; metaphysis and physis. In type V fracture, a small inferior clavicular fragment
scapular rotation; and pull of the tra- remains attached to the CC ligaments.
pezius muscle on the proximal frag-
ment.
these soft-tissue attachments. fragment is detached from the CC
Type III fractures are similar to ligaments. The distal fragment re-
Classification type I fractures in that they also oc- mains attached to the scapula via the
cur distal to the CC ligaments. How- AC joint capsule. In type IIA frac-
Neer5,11 and later, Craig,12 classified ever, type III fracture extends into ture, the fracture lies medial to the
distal third clavicle fractures into the AC joint. Because the ligamen- conoid ligament. In type IIB fracture,
three types based on the relationship tous structures remain intact, type III the fracture lies between the conoid
of the fracture line to the CC liga- fractures are relatively stable and and trapezoid ligaments. The rela-
ments and AC joint (Figure 1). Type typically are minimally displaced. tionship of the distal fragment to the
I fractures occur lateral to the CC Persons with this injury may be at coracoid process may differ between
ligaments but spare the AC joint. risk of posttraumatic AC joint ar- types IIA and IIB.
The proximal fragment is stabilized thropathy because of the intra- In type IIA fractures, the distal
to the coracoid process by the CC articular involvement. fragment remains connected to the
ligaments and to the distal fragment Type II fractures are less stable coracoid process by the CC liga-
by the deltotrapezial fascia. Type I than type I and III fractures, and ments, which are presumed to be in-
fractures often are only minimally they present a treatment challenge. tact. With type IIB fractures, the CC
displaced because of the presence of In all type II fractures, the proximal ligaments lie within the zone of in-
July 2011, Vol 19, No 7 393
Management of Distal Clavicle Fractures
Figure 2 tures were classified as type 3. These
occur lateral to a vertical line drawn
upward from the center of the cora-
coid process. Robinson grouped
fractures into subgroups A and B
based on displacement of the major
fragments. Subtypes A and B were
subdivided according to articular in-
volvement. This classification was
found to have substantial interob-
server reliability (mean kappa value
= 0.77) and excellent intraobserver
reliability (average kappa value =
0.84).
Clinical Evaluation
Most distal clavicle fractures are the
result of a fall onto the distal clavicle
Illustration of the Robinson classification of distal clavicle fractures (type 3). or a direct blow to it.1,16 Direct impact
Type A, cortical alignment fractures: 1, extra-articular; 2, intra-articular. Type occurs at the acromion, usually with
B, displaced fractures: 1, extra-articular; 2, intra-articular. (Redrawn with
permission from Robinson CM: Fractures of the clavicle in the adult:
the arm in an adducted position, and
Epidemiology and classification. J Bone Joint Surg Br 1998;80[3]:476-484.) force is transmitted through the AC
joint to the CC ligaments and the dis-
tal clavicle. Patients with distal clavicle
jury. In Neer type IIB fractures, the taphysis. Depending on the degree of fractures typically present with shoul-
conoid ligament is torn, but the trap- displacement, these patients are der pain. Associated injuries should be
ezoid is presumed to remain attached treated with closed or open reduc- ruled out, such as other injuries to the
to the distal fragment.12 This classifi- tion.14 In type V fracture, only a shoulder girdle, rib fracture, ipsilateral
cation was developed before wide- small inferior cortical fragment re- upper extremity injury, and injury to
spread use of MRI, and we are un- mains attached to the CC ligaments. the thorax or cervical spine. These are
aware of any study that has Type V fractures are functionally particularly likely to occur in conjunc-
confirmed the integrity of the trape- similar to type II injuries in that nei- tion with high-energy mechanisms.
zoid and conoid ligaments in type ther the proximal nor the distal frag- Physical examination findings in-
IIA and IIB injuries. Although in type ment is connected to the coracoid clude swelling, ecchymosis, and ten-
II fractures, fracture displacement process via the CC ligaments. Al- derness over the distal clavicle, as
may be obvious, the exact location though the ligaments may remain at- well as painful active and passive
of the fracture and the integrity of tached to a free-floating bony frag- range of motion (ROM) of the
the CC ligaments may be difficult to ment, the stability of the distal and shoulder. Fracture displacement may
judge on plain radiographs. proximal fracture fragments is com- cause the proximal fragment to tent
Type IV and V fractures were sub- promised. Although the Craig modi- the skin, with an appearance similar
sequently added to the classifica- fication of the Neer classification to that of AC joint separation (Fig-
tion.11 Type IV fractures are rare; system is widely used, no study has ure 3). Paresthesias resulting from
they involve disruption of the perios- assessed the validity of this classifica- swelling or injury to the supraclavic-
teal sleeve in the pediatric popula- tion through inter- and intraobserver ular nerves are common. Neurologic
tion.13,14 These fractures are injuries reliability. examination of the shoulder and up-
to the growth plate in which the Robinson15 proposed an alternative per extremity should be performed
epiphysis and physis typically main- classification for all clavicle fractures and documented. Suprascapular
tain their relationship to the shoulder based on fracture location, displace- nerve injury after distal clavicle frac-
joint, resulting in apparent superior ment, and intra-articular involve- ture has been described.17 Weakness
displacement of the clavicular me- ment (Figure 2). Distal clavicle frac- on external rotation with the arm in
394 Journal of the American Academy of Orthopaedic Surgeons
Rahul Banerjee, MD, et al
Figure 3
A, Clinical photograph of a displaced left distal clavicle fracture in a 21-year-old woman who fell onto her left shoulder.
B, Preoperative AP radiograph demonstrating fracture displacement with no residual cortical contact between the bone
ends. The patient was treated with a distal radius 2.4-mm locking plate and simultaneous coracoclavicular stabilization
using suture. C, AP radiograph obtained 3 months postoperatively demonstrating fracture healing.
adduction and disproportionate re- tal clavicle fractures are typically series used the Neer definition of
ports of pain could be indicative of nondisplaced and heal without diffi- nonunion. Rokito et al7 reported
suprascapular nerve injury. Careful culty with nonsurgical management. nonunion in 7 of 16 patients treated
examination of the remainder of the In contrast, type II fractures are of- nonsurgically for type II distal clavi-
upper extremity, as well as the cervi- ten displaced and may have a higher cle fractures.
cal spine and the thorax, is essential. rate of nonunion.4 Reported rates Risk factors for nonunion include
of nonunion following nonsurgical displacement, that is, no residual cor-
management of type II distal clavi- tical contact between the bone ends,
Radiographic Evaluation
cle fractures range from 28% to and advancing patient age.19 Robin-
Radiographic evaluation should in- 44%1,4,5,7,11,19-21 (Table 1). Most stud- son et al19 noted that both of these
clude true AP and axillary lateral ies define distal clavicle fracture non- factors are independently predictive
views of the shoulder. A Zanca view union based on Neer’s original series. of nonunion.
of the AC joint, which is obtained in Neer defined delayed nonunion as Because some patients remain
10° to 15° cephalic tilt, is also help- “lack of bone bridging for more than asymptomatic, the clinical impor-
ful in evaluating for intra-articular 12 months after injury.”4 This defini- tance of distal clavicle nonunion has
involvement.18 A radiograph show- tion has been used in subsequent been questioned. In the study by
ing the bilateral clavicles and includ- studies on distal clavicle fracture. Deafenbaugh et al,21 none of the
ing the AC joint is useful in assessing Deafenbaugh et al21 reported 3 three reported distal clavicle non-
fracture displacement. These radio- nonunions in a series of 10 Neer type unions was symptomatic. Other
graphs can provide an overall assess- II distal clavicle fractures. Nordqvist studies involving clinical assessment
ment of fracture pattern, location, et al20 reported a 28% nonunion rate of patients with distal clavicular non-
and displacement. (5 of 18). In their review of 43 type unions have indicated that 20% to
II distal clavicle fractures, Edwards 34% were symptomatic and eventu-
Management et al22 noted that up to 75% of pa- ally required surgical fixation.1,20
tients treated nonsurgically devel- Closer evaluation of studies that
Distal clavicle fractures may be man- oped a delayed union or nonunion. included outcomes scores in their
aged nonsurgically or surgically. Of the 20 patients treated nonsurgi- analyses further clarifies the impact
Most nondisplaced distal clavicle cally, 6 (30%) developed nonunion of distal clavicle nonunion. In the
fractures are managed nonsurgically. (ie, lack of bony bridging after 12 small series by Rokito et al,7 7 of the
For example, Neer type I and III dis- months). The authors of these three 16 patients treated nonsurgically de-
July 2011, Vol 19, No 7 395
Management of Distal Clavicle Fractures
Table 1
Reported Rates of Nonunion Following Nonsurgical Management of Type II Distal Clavicle Fractures
No. of Pts With Neer No. of Pts Followed
Study Level of Evidence Total No. of Pts Type II Fracture to End of Study
Neer4 IV (case series) 23 23 23
Deafenbaugh et al21 II (prospective study) 10 10 10
Edwards et al22 IV (case series) 43 43 43c
Nordqvist et al20 IV (case series) 110 23 18d
Rokito et al7 IV (case series) 30 30 30
Robinson and Cairns1 IV (case series) 101 90 86e
Robinson et al19 I (prospective study) 263 99 84g
N/A = not applicable, NR = not reported, ORIF = open reduction and internal fixation, Pts = patients
a
In the nonsurgical group, no fracture was “united by callus prior to 16 weeks after injury.”
b
In the surgical group, “[h]eavy labor was resumed at the third month.”
c
Only 38 patients were reviewed clinically and radiographically. The authors state, “[T]he remaining 5 had adequate case notes and
radiographs.”
d
Only 18 of the 23 patients with Neer type II distal clavicle fractures were evaluated radiographically at final follow-up.
e
86 of the original 101 patients were available for follow-up, but the authors do not specify how many of these were Neer type II clavicle
fractures.
f
This rate is based on all 86 lateral or distal clavicle fractures; the authors do not specify Neer classification.
g
84 lateral end clavicle fractures were followed for 24 weeks. Although 42 fractures were displaced, the number of Neer type II fractures was
not reported.
h
The authors report a 25.4% nonunion rate for displaced lateral end clavicle fractures but an overall nonunion rate of 11.5% (ie, displaced
and nondisplaced).
veloped nonunion, but there was no tal clavicle fractures reflects that of management of closed displaced type
difference in mean Constant or Neer’s original series. (2) Fracture II distal clavicle fracture must be ap-
American Shoulder and Elbow Sur- displacement, as seen in most Neer proached on a case-by-case basis.
geons (ASES) scores between those type II fractures, is associated with
treated nonsurgically and those the development of nonunion. (3) Nonsurgical
treated surgically. In the case series Radiographic nonunion does not al-
Most distal clavicle fractures are
by Robinson and Cairns,1 there was ways correlate with symptomatic
managed nonsurgically. Sling immo-
no significant difference in the Con- nonunion. (4) Patients who develop
bilization for 2 weeks is instituted
stant score or the Medical Outcomes symptomatic nonunion may or may
for comfort, and shoulder motion is
Study 36-Item Short Form score be- not require additional surgery.
initiated as soon as the initial pain
tween any of the three groups stud- Surgical management of distal
ied: patients treated nonsurgically, clavicle fractures is indicated for improves. Repeat radiographs are
patients who developed a nonunion, open fractures, skin compromise, obtained at 6-week follow-up to
and patients who underwent delayed and associated vascular injury re- monitor for fracture displacement
surgical treatment after the develop- quiring surgery. Because of the high and evidence of healing. These pa-
ment of a nonunion. rate of nonunion, Neer4 and tients typically recover fully without
Based on these data, several con- others2,3,6,23-45 have advocated pri- sequelae. Type I and type III frac-
clusions may be reached regarding mary surgical management of distal tures are at risk of delayed-onset
nonunion after distal clavicle frac- clavicle fracture. However, because symptomatic AC arthrosis,5 which
ture: (1) The reported rate of radio- radiographic nonunion does not cor- can be managed with distal clavicle
graphic nonunion of all types of dis- relate with symptomatic nonunion, resection, if necessary. Nondisplaced
396 Journal of the American Academy of Orthopaedic Surgeons
Rahul Banerjee, MD, et al
Table 1 (continued)
Reported Rates of Nonunion Following Nonsurgical Management of Type II Distal Clavicle Fractures
No. of Symptomatic
Management Average Follow-up Outcome Nonunions
12 nonsurgical 4 moa 8 delayed union (67%), 4
4 nonunion (33%)
4 excision NR N/A NR
7 ORIF 3 mob All united 0
Nonsurgical 14.3 mo 3 nonunion (30%) 0
20 nonsurgical 3y 9 delayed union (45%), 6
6 nonunion (30%)
23 surgical 21 mo All united 0
Nonsurgical 15 y 5/18 nonunion (28%) 2
16 nonsurgical 53.5 mo 7 nonunion (44%) 2
14 ORIF 59.8 mo All united 0
72 nonsurgical, 3 excision, 6.2 y 32/86 nonunion (37%)f 11
11 delayed surgery
Nonsurgical 24 wk 25.4% nonunionh NR
N/A = not applicable, NR = not reported, ORIF = open reduction and internal fixation, Pts = patients
a
In the nonsurgical group, no fracture was “united by callus prior to 16 weeks after injury.”
b
In the surgical group, “[h]eavy labor was resumed at the third month.”
c
Only 38 patients were reviewed clinically and radiographically. The authors state, “[T]he remaining 5 had adequate case notes and
radiographs.”
d
Only 18 of the 23 patients with Neer type II distal clavicle fractures were evaluated radiographically at final follow-up.
e
86 of the original 101 patients were available for follow-up, but the authors do not specify how many of these were Neer type II clavicle
fractures.
f
This rate is based on all 86 lateral or distal clavicle fractures; the authors do not specify Neer classification.
g
84 lateral end clavicle fractures were followed for 24 weeks. Although 42 fractures were displaced, the number of Neer type II fractures was
not reported.
h
The authors report a 25.4% nonunion rate for displaced lateral end clavicle fractures but an overall nonunion rate of 11.5% (ie, displaced
and nondisplaced).
type II fractures may also be man- tions, including nonunion, AC decrease complications.24-26
aged nonsurgically. However, the arthrosis, and Kirschner wire (K- CC ligament repair or reconstruc-
likelihood of subsequent displace- wire) migration. Although Eskola tion without supplemental fixation
ment and possible nonunion should et al46 reported good or satisfactory has been reported.6,27 Webber and
be recognized, discussed with the pa- outcomes in 22 of 23 patients, 26% Haines6 described CC ligament re-
tient, and monitored with repeat ra- experienced a complication or non- construction using a Dacron graft in
diographs at 6 weeks. union following transacromial wir- 11 patients. All fractures united by
ing. Late migration of the wires into an average of 43.5 days postopera-
Surgical the cervical spine, trachea, vascular tively. At a mean follow-up of 4.6
A variety of methods of surgical structures, lung, and abdomen has years, the average Constant score
management of distal clavicle frac- been reported.47-49 Modifications was 98.9.
tures has been proposed, including have led to a reduction in unsatisfac- The modified Weaver-Dunn proce-
transacromial wire fixation, a modi- tory results and complications asso- dure is primarily used for AC dislo-
fied Weaver-Dunn procedure, use ciated with transacromial wire fixa- cation, but it also has been advo-
of a tension band, CC screw fixa- tion. Good results have been cated for the management of distal
tion, plate fixation, and arthro- reported with the use of a transacro- clavicle fractures.50 This procedure is
scopic treatment. Neer4 recom- mial Knowles pin rather than usually reserved for cases in which
mended transacromial wire fixation K-wires.23,24 Transacromial fixation the distal clavicle fragment can be
of distal clavicle fractures. This com- supplemented with CC ligament easily excised and the coracoacro-
monly used technique has been asso- repair or reconstruction has also mial ligament can be transferred
ciated with a high rate of complica- been shown to improve results and to the distal end of the proximal
July 2011, Vol 19, No 7 397
Management of Distal Clavicle Fractures
Figure 4
A, AP radiograph of the right shoulder in a 56-year-old woman who sustained a closed distal clavicle fracture after a
fall. B, The patient was initially treated nonsurgically and developed painful nonunion. She then underwent fixation with
a 2.7-mm plate, which allowed placement of three screws into the distal fragment. The fixation was augmented with
coracoclavicular stabilization using Mersilene tape. AP radiograph (C) and postoperative photographs (D through G)
obtained 3 months postoperatively demonstrating healing and return to preinjury level of function.
clavicle fragment. to the coracoid process. Successful clavicle fragment. All eight patients
K-wire fixation with a supplemen- healing of the distal clavicle has been who were available for follow-up
tary tension band wire has also been reported in several small case achieved bony union. The mean
suggested for fixation of type II dis- series.22,32-34 This technique has also Constant score was 96.
tal clavicle fractures.51 In this been performed using a cannulated If the distal fragment is too small
method, K-wires are placed on the screw.35 More recently, Fazal et al36 to hold screws, a plate that hooks
superior aspect of the clavicle, avoid- reported a 100% union rate using under the acromion may be used
ing the AC joint. The tension band is this technique in 30 patients. A sec- (Figure 5). Kashii et al38 reported on
placed around the wires. In one se- ond procedure is required to remove 34 patients with distal clavicle frac-
ries, 11 of 12 patients achieved pain- the screw following union. tures treated with an AC hook plate.
less union with this approach.52 Oth- Small and mini-fragment locking Although all patients achieved bony
ers have reported similar success plates may be used to stabilize distal union, the hook caused acromial
rates with modified tension band clavicle fractures (Figures 3 and 4). fracture in one patient and rotator
techniques using suture.28-30 Symp- These plates allow fixation of the cuff tear in another. Good union
tomatic hardware is a potential com- distal clavicle fragment without rates with the hook plate were re-
plication, particularly when tension crossing the AC joint. Kalamaras ported in two other studies, but
band wiring is used.31 et al37 used a distal radius locking asymptomatic osteolysis of the acro-
In CC screw fixation, open reduc- plate on nine patients with distal mion and migration of the hook into
tion and internal fixation of the dis- clavicle fracture. The 2.4-mm lock- the acromion were frequently en-
tal clavicle fragment is performed by ing screws in the distal portion of the countered.39,40 With the hook plate, a
temporarily fixing the distal clavicle plate were used to capture the distal second procedure is required for
398 Journal of the American Academy of Orthopaedic Surgeons
Rahul Banerjee, MD, et al
Figure 5 initiated. When pain has improved
and there are early signs of fracture
consolidation, active ROM is al-
lowed.
For the patient with displaced type
II distal clavicle fracture or displaced
type IV or V fracture, treatment se-
lection is based on the degree of dis-
placement and a discussion with the
patient. Robinson et al19 defined dis-
placement (ie, no residual cortical
contact between the bone ends) as a
A, AP radiograph of the right shoulder in a 60-year-old man who sustained a risk factor for nonunion. For pa-
displaced distal clavicle fracture in a fall. He was treated with open reduction
and internal fixation using a distal clavicle hook plate. B, AP radiograph tients with displacement, we offer
obtained 5 months postoperatively demonstrating fracture healing. The plate surgical treatment but counsel them
was removed 9 months postoperatively. that the current evidence suggests
equivalent outcomes between surgi-
cal and nonsurgical treatment.
plate removal, which may cause ad- retrospectively compared K-wire fix- Our preferred surgical manage-
ditional morbidity. ation with the use of a clavicular ment technique is internal fixation of
Plate fixation may be supple- hook plate (22 and 17 patients, re- the distal clavicle fracture with sup-
mented with CC screw fixation spectively). Although both methods plementary CC fixation (Figures 3
through the plate or with CC liga- restored shoulder function, K-wire and 4). If the distal clavicle fragment
ment repair or reconstruction. Sup- fixation was associated with wire mi- is large enough to hold screws, we
plemental CC fixation may also be gration in 12 patients, loss of reduc- use a small, low-profile locking plate
achieved with sutures or suture an- tion in 7, infection in 3, and non- and perform open anatomic fracture
chors. Recently, Herrmann et al3 de- union in 2. In the group treated with reduction. The coracoid process is
scribed the use of a locking T-plate in clavicle hook plates, one patient sus- identified to allow for suture pas-
addition to suture anchors placed sage. The fixation is supple-
tained a clavicle fracture, and two
into the coracoid in eight patients. mented by CC stabilization, which is
fractures went on to nonunion. More
The sutures were placed around the achieved with sutures placed around
recently, Lee et al31 retrospectively re-
clavicle and over the plate. Bony the coracoid process and either
viewed patients treated with either
union was achieved in 6 weeks in the around or through a small hole in
clavicular hook plates or tension-
seven patients who were available the clavicle, proximal to the fracture.
band wiring (32 and 20 patients, re-
for follow-up; the mean Constant For cases in which the size or qual-
spectively). Hook plating was associ-
score was 93.3. ity of the distal fracture fragment is
ated with a lower complication rate
Arthroscopic techniques for the insufficient for plate application, we
and a lower rate of symptomatic
management of distal clavicle frac- recommend CC stabilization using
hardware. In addition, it better facili-
tures have also been reported. These nonabsorbable suture such as Ethi-
tated return to work and athletic ac-
techniques employ some of the same bond (Ethicon, Somerville, NJ), Fi-
tivity.
strategies used in arthroscopically as- berWire (Arthrex, Naples, FL), or
sisted CC ligament reconstruction Mersilene (Ethicon). This approach
following AC joint separation. Pub- Authors’ Preferred requires exposure of the coracoid
lished reports are limited to small Management process. Two strands of suture are
case series and technical notes, and passed around the coracoid process.
all involve arthroscopic CC stabiliza- We recommend primary nonsurgical The ends of the suture are then
tion using suture, a double-button management of type I, type III, and passed through a small drill hole in
device, or the Tightrope system (Ar- nondisplaced type II distal clavicle the proximal clavicle fragment. The
threx, Naples, FL).41-44 fractures. Patients are treated with distal clavicle is reduced, and the
Only two studies to date have di- sling immobilization for 2 weeks. first suture is tied. Once reduction is
rectly compared two methods of sur- During this period, supine passive confirmed visually and radiographi-
gical management. Flinkkilä et al45 ROM and active-assisted ROM are cally, the second suture is tied. The
July 2011, Vol 19, No 7 399
Management of Distal Clavicle Fractures
fixation is supplemented by a dorsal 16, 20, 22-30, 32-40, 43, 44, and 52 13. Katznelson A, Nerubay J, Oliver S:
Dynamic fixation of the avulsed clavicle.
suture tension band placed through are level IV studies. Reference 10 is J Trauma 1976;16(10):841-844.
the incision, as described by Levy.30 level V expert opinion.
14. Ogden JA: Distal clavicular physeal
Surgeons who are trained in shoulder References printed in bold type indi- injury. Clin Orthop Relat Res 1984;
arthroscopy may perform the proce- cate those published within the past (188):68-73.
dure arthroscopically. 5 years. 15. Robinson CM: Fractures of the clavicle
Postoperatively, the patient is in the adult: Epidemiology and
1. Robinson CM, Cairns DA: Primary classification. J Bone Joint Surg Br 1998;
placed in a sling for 6 weeks. Supine nonoperative treatment of displaced 80(3):476-484.
passive and active-assisted ROM ex- lateral fractures of the clavicle. J Bone
Joint Surg Am 2004;86(4):778-782. 16. Stanley D, Trowbridge EA, Norris SH:
ercises are begun immediately. Active The mechanism of clavicular fracture: A
ROM is started at 6 weeks, with 2. Hessmann M, Kirchner R, Baumgaertel clinical and biomechanical analysis.
F, Gehling H, Gotzen L: Treatment of J Bone Joint Surg Br 1988;70(3):461-
progression to strengthening exer- unstable distal clavicular fractures with 464.
cises 6 to 12 weeks postoperatively. and without lesions of the acromio-
clavicular joint. Injury 1996;27(1):47- 17. Huang KC, Tu YK, Huang TJ, Hsu RW:
Patients are typically restricted from Suprascapular neuropathy complicating
52.
engaging in heavy labor and sports a Neer type I distal clavicular fracture: A
3. Herrmann S, Schmidmaier G, Greiner S: case report. J Orthop Trauma 2005;
for 12 weeks.
Stabilisation of vertical unstable distal 19(5):343-345.
clavicular fractures (Neer 2b) using
locking T-plates and suture anchors. 18. Zanca P: Shoulder pain: Involvement of
the acromioclavicular joint: Analysis of
Summary Injury 2009;40(3):236-239.
1,000 cases. Am J Roentgenol Radium
4. Neer CS II: Fracture of the distal clavicle Ther Nucl Med 1971;112(3):493-506.
Most distal clavicle fractures may be with detachment of the coracoclavicular
ligaments in adults. J Trauma 1963;3:99- 19. Robinson CM, Court-Brown CM,
managed nonsurgically. Type II distal McQueen MM, Wakefield AE:
110.
clavicle fractures are associated with Estimating the risk of nonunion
5. Neer CS II: Fractures of the distal third following nonoperative treatment of a
radiographic nonunion in up to 44% of the clavicle. Clin Orthop Relat Res clavicular fracture. J Bone Joint Surg Am
of cases. Fracture displacement is as- 1968;58:43-50. 2004;86(7):1359-1365.
sociated with a higher risk of non- 6. Webber MC, Haines JF: The treatment 20. Nordqvist A, Petersson C, Redlund-
union. However, the clinical rele- of lateral clavicle fractures. Injury 2000; Johnell I: The natural course of lateral
31(3):175-179. clavicle fracture: 15 (11-21) year
vance of this nonunion may be follow-up of 110 cases. Acta Orthop
minimal, and initial nonsurgical 7. Rokito AS, Zuckerman JD, Shaari JM, Scand 1993;64(1):87-91.
Eisenberg DP, Cuomo F, Gallagher MA:
management may be warranted. Al- A comparison of nonoperative and 21. Deafenbaugh MK, Dugdale TW, Staeheli
though surgical management of distal operative treatment of type II distal JW, Nielsen R: Nonoperative treatment
clavicle fractures. Bull Hosp Jt Dis 2002- of Neer type II distal clavicle fractures: A
clavicle fractures has been described, 2003;61(1-2):32-39. prospective study. Contemp Orthop
current evidence suggests equivalent 1990;20(4):405-413.
8. Fukuda K, Craig EV, An KN, Cofield
outcomes between surgical and nonsur- RH, Chao EY: Biomechanical study of 22. Edwards DJ, Kavanagh TG, Flannery
gical management. Additionally, no the ligamentous system of the MC: Fractures of the distal clavicle: A
acromioclavicular joint. J Bone Joint case for fixation. Injury 1992;23(1):44-
single surgical technique has been Surg Am 1986;68(3):434-440. 46.
shown to be superior to the others. A
9. Renfree KJ, Riley MK, Wheeler D, Hentz 23. Fann CY, Chiu FY, Chuang TY, Chen
prospective randomized study compar- JG, Wright TW: Ligamentous anatomy CM, Chen TH: Transacromial Knowles
ing surgical and nonsurgical manage- of the distal clavicle. J Shoulder Elbow pin in the treatment of Neer type 2 distal
Surg 2003;12(4):355-359. clavicle fractures: A prospective
ment of type II distal clavicle fractures evaluation of 32 cases. J Trauma 2004;
is necessary to better determine the op- 10. Bearden JM, Hughston JC, Whatley GS: 56(5):1102-1105.
Acromioclavicular dislocation: Method
timal treatment. of treatment. J Sports Med 1973;1(4):5- 24. Wang SJ, Wong CS: Extra-articular
17. knowles pin fixation for unstable distal
clavicle fractures. J Trauma 2008;64(6):
11. Neer C II: Fractures and dislocations of 1522-1527.
References the shoulder, in Rockwood CA Jr, Green
DP, eds: Fractures in Adults. Philadel- 25. Bezer M, Aydin N, Guven O: The
phia, PA, J.B. Lippincott, 1984, pp 711- treatment of distal clavicle fractures with
Evidence-based Medicine: Levels of 712. coracoclavicular ligament disruption: A
evidence are listed in the table of report of 10 cases. J Orthop Trauma
12. Craig EV: Fractures of the clavicle, in 2005;19(8):524-528.
contents. In this article, reference 19 is Rockwood CA Jr, Green DP, Bucholz
a level I study. Reference 21 is a level II RW, Heckman JD, eds: Rockwood and 26. Chen CH, Chen WJ, Shih CH: Surgical
Green’s Fractures in Adults, ed 4. treatment for distal clavicle fracture with
study. References 31 and 45 are level Philadelphia, PA, Lippincott-Raven, coracoclavicular ligament disruption.
III studies. References 1-7, 13, 14, 1996, pp 1109-1193. J Trauma 2002;52(1):72-78.
400 Journal of the American Academy of Orthopaedic Surgeons
Rahul Banerjee, MD, et al
27. Goldberg JA, Bruce WJ, Sonnabend DH, screw fixation technique. J Trauma Arthroscopic treatment of distal clavicle
Walsh WR: Type 2 fractures of the distal 2006;60(6):1358-1361. fractures: A technical note. Knee Surg
clavicle: A new surgical technique. Sports Traumatol Arthrosc 2008;16(9):
J Shoulder Elbow Surg 1997;6(4):380- 36. Fazal MA, Saksena J, Haddad FS: 884-886.
382. Temporary coracoclavicular screw
fixation for displaced distal clavicle 45. Flinkkilä T, Ristiniemi J, Hyvönen P,
28. Mall JW, Jacobi CA, Philipp AW, Peter fractures. J Orthop Surg (Hong Kong) Hämäläinen M: Surgical treatment of
FJ: Surgical treatment of fractures of the 2007;15(1):9-11. unstable fractures of the distal clavicle: A
distal clavicle with polydioxanone suture comparative study of Kirschner wire and
tension band wiring: An alternative 37. Kalamaras M, Cutbush K, Robinson M:
clavicular hook plate fixation. Acta
osteosynthesis. J Orthop Sci 2002;7(5): A method for internal fixation of
Orthop Scand 2002;73(1):50-53.
535-537. unstable distal clavicle fractures: Early
observations using a new technique. 46. Eskola A, Vainionpää S, Pätiälä H,
29. Badhe SP, Lawrence TM, Clark DI: J Shoulder Elbow Surg 2008;17(1):60-
Tension band suturing for the treatment Rokkanen P: Outcome of operative
62. treatment in fresh lateral clavicular
of displaced type 2 lateral end clavicle
fractures. Arch Orthop Trauma Surg 38. Kashii M, Inui H, Yamamoto K: Surgical fracture. Ann Chir Gynaecol 1987;76(3):
2007;127(1):25-28. treatment of distal clavicle fractures 167-169.
using the clavicular hook plate. Clin
30. Levy O: Simple, minimally invasive 47. Regel JP, Pospiech J, Aalders TA,
Orthop Relat Res 2006;447:158-164.
surgical technique for treatment of type Ruchholtz S: Intraspinal migration of a
2 fractures of the distal clavicle. 39. Tambe AD, Motkur P, Qamar A, Drew Kirschner wire 3 months after clavicular
J Shoulder Elbow Surg 2003;12(1):24- S, Turner SM: Fractures of the distal fracture fixation. Neurosurg Rev 2002;
28. third of the clavicle treated by hook 25(1-2):110-112.
plating. Int Orthop 2006;30(1):7-10.
31. Lee YS, Lau MJ, Tseng YC, Chen WC, 48. Tsai CH, Hsu HC, Huan CY, Chen HT,
Kao HY, Wei JD: Comparison of the 40. Muramatsu K, Shigetomi M, Matsunaga Fong YC: Late migration of threaded
efficacy of hook plate versus tension T, Murata Y, Taguchi T: Use of the AO wire (schanz screw) from right distal
band wire in the treatment of unstable hook-plate for treatment of unstable clavicle to the cervical spine. J Chin Med
fractures of the distal clavicle. Int fractures of the distal clavicle. Arch Assoc 2009;72(1):48-51.
Orthop 2009;33(5):1401-1405. Orthop Trauma Surg 2007;127(3):191-
194. 49. Lyons FA, Rockwood CA Jr: Migration
32. Ballmer FT, Gerber C: Coracoclavicular
of pins used in operations on the
screw fixation for unstable fractures of 41. Nourissat G, Kakuda C, Dumontier C,
shoulder. J Bone Joint Surg Am 1990;
the distal clavicle: A report of five cases. Sautet A, Doursounian L: Arthroscopic
72(8):1262-1267.
J Bone Joint Surg Br 1991;73(2):291- stabilization of Neer type 2 fracture of
294. the distal part of the clavicle. 50. Anderson K: Evaluation and treatment
Arthroscopy 2007;23(6):674.e1-4. of distal clavicle fractures. Clin Sports
33. Yamaguchi H, Arakawa H, Kobayashi
M: Results of the Bosworth method for 42. Baumgarten KM: Arthroscopic fixation Med 2003;22(2):319-326, vii.
unstable fractures of the distal clavicle. of a type II-variant, unstable distal
51. Heim U, Pfeiffer KM: Internal Fixation
Int Orthop 1998;22(6):366-368. clavicle fracture. Orthopedics 2008;
of Small Fractures: Technique
31(12):pii:orthosupersite.com/
34. Macheras G, Kateros KT, Savvidou OD, Recommended by the AO-ASIF Group,
view.asp?rID=32937.
Sofianos J, Fawzy EA, Papagelopoulos ed 3. New York, NY, Springer-Verlag,
PJ: Coracoclavicular screw fixation for 43. Checchia SL, Doneux PS, Miyazaki AN, 1987.
unstable distal clavicle fractures. Fregoneze M, Silva LA: Treatment of
Orthopedics 2005;28(7):693-696. distal clavicle fractures using an 52. Kao FC, Chao EK, Chen CH, Yu SW,
arthroscopic technique. J Shoulder Chen CY, Yen CY: Treatment of distal
35. Jin CZ, Kim HK, Min BH: Surgical Elbow Surg 2008;17(3):395-398. clavicle fracture using Kirschner wires
treatment for distal clavicle fracture and tension-band wires. J Trauma 2001;
associated with coracoclavicular 44. Pujol N, Philippeau JM, Richou J, 51(3):522-525.
ligament rupture using a cannulated Lespagnol F, Graveleau N, Hardy P:
July 2011, Vol 19, No 7 401
You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Transference Focused PsychotherapyDocument22 pagesTransference Focused PsychotherapybobifilNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Milling and Grain Magazine - July 2015 - FULL EDITIONDocument104 pagesMilling and Grain Magazine - July 2015 - FULL EDITIONMilling and Grain magazineNo ratings yet
- OU Shoulder and Elbow OITE Review: September 23, 2015 Betsy M. Nolan MDDocument159 pagesOU Shoulder and Elbow OITE Review: September 23, 2015 Betsy M. Nolan MDJayNo ratings yet
- TrihexyphenidylDocument2 pagesTrihexyphenidylArnzz Agbulos50% (2)
- 2017 OITE ReviewDocument105 pages2017 OITE ReviewJayNo ratings yet
- Salient Features of Ra 10121Document47 pagesSalient Features of Ra 10121shella.msem100% (2)
- MORE 1119 Module For Remedial English SPM 1119 160616 1Document191 pagesMORE 1119 Module For Remedial English SPM 1119 160616 1Qing Yi100% (3)
- Orthopedic OITE Info Version 1enDocument2 pagesOrthopedic OITE Info Version 1enJay100% (1)
- Spinal Cord Injury Garstang 10-16-09 GrayscaleDocument12 pagesSpinal Cord Injury Garstang 10-16-09 GrayscaleJayNo ratings yet
- Intramedullary Nailing of Pediatric Femoral Shaft FractureDocument10 pagesIntramedullary Nailing of Pediatric Femoral Shaft FractureJayNo ratings yet
- NICE ProceedingsDocument63 pagesNICE Proceedingssn_b5No ratings yet
- Surgical Positions and Incisions Surgical Procedure Surgical Incision Surgical Position Nursing Responsibilities and PrecautionsDocument3 pagesSurgical Positions and Incisions Surgical Procedure Surgical Incision Surgical Position Nursing Responsibilities and PrecautionsCatherine PradoNo ratings yet
- Group 5 13B: End Stage Renal Failure Secondary To Diabetes NephropathyDocument68 pagesGroup 5 13B: End Stage Renal Failure Secondary To Diabetes NephropathyJinski007100% (1)
- Codex Alimentarius PDFDocument71 pagesCodex Alimentarius PDFMelo MassionaNo ratings yet
- Managing Latent Tuberculosis Managing Latent Tuberculosis: NICE Pathway Last Updated: 12 September 2019Document10 pagesManaging Latent Tuberculosis Managing Latent Tuberculosis: NICE Pathway Last Updated: 12 September 2019Fabric MacNo ratings yet
- BrainwashedDocument2 pagesBrainwashedapi-304543250No ratings yet
- Cholesterol, Triglycerides, and Associated Lipoproteins - Clinical Methods - NCBI BookshelfDocument30 pagesCholesterol, Triglycerides, and Associated Lipoproteins - Clinical Methods - NCBI BookshelfNeha MasarkarNo ratings yet
- LoE in APAC 2012magazineDocument4 pagesLoE in APAC 2012magazineJohn Xi Zhen HuanNo ratings yet
- MS Gi7Document5 pagesMS Gi7Amiel Francisco ReyesNo ratings yet
- Week 3-Fringe Benefit TaxDocument51 pagesWeek 3-Fringe Benefit TaxMARCIAL, Althea Kate A.No ratings yet
- Tutorial 12Document2 pagesTutorial 12Eva EvangelineNo ratings yet
- Fundamentals of StisDocument2 pagesFundamentals of Stisapi-646865632No ratings yet
- Sop Chlorine and Ammonia GasesDocument3 pagesSop Chlorine and Ammonia GasesSE ESTNo ratings yet
- Lecture-Npos in The PhilippinesDocument14 pagesLecture-Npos in The PhilippinesAngela PaduaNo ratings yet
- Family SehatDocument1 pageFamily SehatRaheel KhanNo ratings yet
- NCM 110 - Activity 3Document6 pagesNCM 110 - Activity 3Crisheila Sarah PiedadNo ratings yet
- ArdsDocument29 pagesArdsAmani KayedNo ratings yet
- Gender GenocideDocument19 pagesGender GenocideZAHEERABBASzamNo ratings yet
- 11) ECG Pearls-Diagnosis You Don't Want To Miss - Dr. Noel ThomasDocument104 pages11) ECG Pearls-Diagnosis You Don't Want To Miss - Dr. Noel ThomasAbu Umayr100% (1)
- Dhaval Engineering Company: Blinding and De-Blinding JobDocument2 pagesDhaval Engineering Company: Blinding and De-Blinding JobKumar KushNo ratings yet
- MSEB - Claim - Form 2016 MahaGencoDocument2 pagesMSEB - Claim - Form 2016 MahaGencoAnonymous pKsr5vNo ratings yet
- JSPL Sustainability Report 2014 15Document65 pagesJSPL Sustainability Report 2014 15Vibhash RastogiNo ratings yet
- Hope 3 Week 1 ModulesDocument9 pagesHope 3 Week 1 ModulesPearl Arianne Moncada MontealegreNo ratings yet
- Jerwin JournalDocument3 pagesJerwin JournaljerwiNo ratings yet
- Daftar Harga Farma Dan Otc 13 Juli 2022Document159 pagesDaftar Harga Farma Dan Otc 13 Juli 2022Durrah Zati YumnaNo ratings yet