You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- EpidemiologyDocument3 pagesEpidemiologyAya VirtucioNo ratings yet
- Nursing EmpowermentDocument8 pagesNursing EmpowermentmeityNo ratings yet
- National Vector Borne Disease Control ProgrammeDocument100 pagesNational Vector Borne Disease Control ProgrammeThe ThemerNo ratings yet
- The Added Value of Clinical Hypnosis To FND Treatment: DR Jason Price Consultant Clinical NeuropsychologistDocument21 pagesThe Added Value of Clinical Hypnosis To FND Treatment: DR Jason Price Consultant Clinical Neuropsychologistmeity100% (1)
- JBI-Reviewers Manual-2011 HR PDFDocument201 pagesJBI-Reviewers Manual-2011 HR PDFmeityNo ratings yet
- Policy Brief ABHR ConsultationDocument9 pagesPolicy Brief ABHR ConsultationmeityNo ratings yet
- ESCAP - Policy - Brief (COVID-19 - and - PWDS) PDFDocument4 pagesESCAP - Policy - Brief (COVID-19 - and - PWDS) PDFmeityNo ratings yet
- Statistical AlgorithmsDocument11 pagesStatistical AlgorithmsmeityNo ratings yet
- Whohivtb Policy PDFDocument8 pagesWhohivtb Policy PDFmeityNo ratings yet
- UHC QI Policy BriefDocument2 pagesUHC QI Policy BriefmeityNo ratings yet
- Statistical Algorithms CalculatorDocument7 pagesStatistical Algorithms CalculatormeityNo ratings yet
- Jurnal Kritik Riset Statistik Meity Patient - Safety - Culture - AssociaDocument10 pagesJurnal Kritik Riset Statistik Meity Patient - Safety - Culture - AssociameityNo ratings yet
- Statistical Algorithms CalculatorDocument7 pagesStatistical Algorithms CalculatormeityNo ratings yet
- JBC Form CritAp ExpDocument1 pageJBC Form CritAp ExpIntan Kusuma DewiNo ratings yet
- RM 5 UserguideDocument105 pagesRM 5 UserguidemeityNo ratings yet
- Footnote Link Nic NocDocument5 pagesFootnote Link Nic NocGhea Tahara SugiantoNo ratings yet
- MixedMethods Research Handout PDFDocument17 pagesMixedMethods Research Handout PDFmeityNo ratings yet
- PROF AZADEH Nursing Professionals Breast Cancer PreventionDocument43 pagesPROF AZADEH Nursing Professionals Breast Cancer PreventionmeityNo ratings yet
- Tugas LTM Dan Populasi Sampel DGDocument12 pagesTugas LTM Dan Populasi Sampel DGmeityNo ratings yet
- Patient SafetyDocument6 pagesPatient SafetymeityNo ratings yet
- Patient Safety Culture NurseDocument104 pagesPatient Safety Culture NursemeityNo ratings yet
- Lecture-Research Report Writing-SsDocument67 pagesLecture-Research Report Writing-SsmeityNo ratings yet
- Introduction To Qualitative Data Analysis Software: Sub TopicsDocument10 pagesIntroduction To Qualitative Data Analysis Software: Sub TopicsmeityNo ratings yet
- 2016 WHO-CIOMS Ethical GuidelinesDocument119 pages2016 WHO-CIOMS Ethical Guidelinesyulianto dwi pamadiNo ratings yet
- A) Immunization B) Vaccination C) Attenuation D) None of TheseDocument4 pagesA) Immunization B) Vaccination C) Attenuation D) None of TheseYadav rupeshNo ratings yet
- (1980) Approved Lists of Bacterial NamesDocument196 pages(1980) Approved Lists of Bacterial NamesLeonardo LopesNo ratings yet
- Antibiotic Susceptibility TestingDocument46 pagesAntibiotic Susceptibility Testingditta antNo ratings yet
- Brochure DiseaseDocument2 pagesBrochure Diseaseapi-295870217No ratings yet
- Biocontrol Activity of Bacillus Against A GFP-marked Pseudomonas Syringae Pv. Tomato On Tomato PhylloplaneDocument11 pagesBiocontrol Activity of Bacillus Against A GFP-marked Pseudomonas Syringae Pv. Tomato On Tomato PhylloplaneRoberto Lanna FilhoNo ratings yet
- Viral Gastroenteritis-1Document17 pagesViral Gastroenteritis-1Abdus SubhanNo ratings yet
- Cellulitis and Skin Abscess in Adults - Treatment - UpToDateDocument16 pagesCellulitis and Skin Abscess in Adults - Treatment - UpToDateIsabella Gutierrez CarabaliNo ratings yet
- The Solution: TICKPLEX®: Multiplex Format: Multi-Functional: Highly Sensitive DetectionDocument2 pagesThe Solution: TICKPLEX®: Multiplex Format: Multi-Functional: Highly Sensitive DetectionTsvetlena IlievaNo ratings yet
- HSB Pneumonia Antibiotic AlgorithmDocument4 pagesHSB Pneumonia Antibiotic AlgorithmDr.Senthil KumarNo ratings yet
- Platelia Dengue Ns1 Ag 1Document114 pagesPlatelia Dengue Ns1 Ag 1Liroense RodpNo ratings yet
- 較常使用之乳酸桿菌屬菌種學名變更對照表Document1 page較常使用之乳酸桿菌屬菌種學名變更對照表YS LNo ratings yet
- CDC Surveilance 2018Document321 pagesCDC Surveilance 2018spiderNo ratings yet
- Putting On and Removing Ppe Diagram - March 2020Document2 pagesPutting On and Removing Ppe Diagram - March 2020Perdana DialisisNo ratings yet
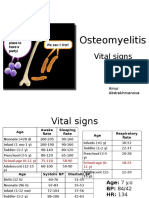
- PBL 2 - OsteomyelitisDocument10 pagesPBL 2 - OsteomyelitisAinur AbdrakhmanovaNo ratings yet
- Nursingcrib Com NURSING CARE PLAN Chicken Pox PDFDocument2 pagesNursingcrib Com NURSING CARE PLAN Chicken Pox PDFAkeroNo ratings yet
- Rusu Maria - MI (020) - PCR (8473781) 29.01.2022 18.23.23Document1 pageRusu Maria - MI (020) - PCR (8473781) 29.01.2022 18.23.23Cristina BurlacuNo ratings yet
- HIV PrognosisDocument16 pagesHIV PrognosisGrace Yuni Soesanti MhNo ratings yet
- Communicable Diseases Chart With PicsDocument3 pagesCommunicable Diseases Chart With PicsesmirikNo ratings yet
- Bacterial Sexually Transmitted Infections: Patrick KimmittDocument77 pagesBacterial Sexually Transmitted Infections: Patrick KimmittJohir ChowdhuryNo ratings yet
- Mycoplasma Hyorhinis Infection of Pigs SINSUI2010 02 A Rovira Et AlDocument8 pagesMycoplasma Hyorhinis Infection of Pigs SINSUI2010 02 A Rovira Et AlAndre BroesNo ratings yet
- 2020 Pharmacology & Therapeutics Pharmacological Targets and Emerging Treatments For Respiratory Syncytial Virus BronchiolitisDocument18 pages2020 Pharmacology & Therapeutics Pharmacological Targets and Emerging Treatments For Respiratory Syncytial Virus BronchiolitisMayra Concha OstosNo ratings yet
- Organism Staining OsceDocument105 pagesOrganism Staining OsceNachchakorn DellNo ratings yet
- Benefits and Limitations of Maldi Tof Mass Spectrometry For The Identification of Microorganisms Journal of Infectiology 1 1142Document5 pagesBenefits and Limitations of Maldi Tof Mass Spectrometry For The Identification of Microorganisms Journal of Infectiology 1 1142ntnquynhproNo ratings yet
- Typhoid FeverDocument8 pagesTyphoid FeverMARIANTO PUTRA SUHARDINo ratings yet
- Faktor - Faktor Yang Mempengaruhi Kejadian Penyakit Demam Berdarah Dengue (DBD) Dan Jenis Serotipe Virus Dengue Di Kabupaten SemarangDocument7 pagesFaktor - Faktor Yang Mempengaruhi Kejadian Penyakit Demam Berdarah Dengue (DBD) Dan Jenis Serotipe Virus Dengue Di Kabupaten SemarangbellaaNo ratings yet
- Microbes NotesDocument22 pagesMicrobes Notesapi-218511741100% (1)
- Center For Food Security and Public Health, Iowa State University, 2011Document35 pagesCenter For Food Security and Public Health, Iowa State University, 2011life hacks every informationNo ratings yet
- A Survey On The Awareness of PneumoniaDocument2 pagesA Survey On The Awareness of PneumoniaAshy LeeNo ratings yet