You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5811)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- CS Form No. 212 Revised Personal Data SheetDocument5 pagesCS Form No. 212 Revised Personal Data SheetKim Rose Sabuclalao85% (13)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Nurse Patient InteractionDocument14 pagesNurse Patient InteractionIris Caberte96% (56)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Policy of Prescription PadDocument2 pagesPolicy of Prescription PaddmuscleNo ratings yet
- Ritu ResumeDocument2 pagesRitu ResumerituNo ratings yet
- FTE Computation - Fiscal Management in Nursing Administration v3Document8 pagesFTE Computation - Fiscal Management in Nursing Administration v3Omar Christian TuazonNo ratings yet
- Reflective Journaling2Document3 pagesReflective Journaling2api-313631358No ratings yet
- Nursing Home Discharge SummaryDocument2 pagesNursing Home Discharge Summarykatemartin217No ratings yet
- Acute Glomerulonephritis 42-mDocument27 pagesAcute Glomerulonephritis 42-mcbanguisNo ratings yet
- Knowledge and Practices of Nurses in Infection Prevention and Control Within A Tertiary Care HospitalDocument4 pagesKnowledge and Practices of Nurses in Infection Prevention and Control Within A Tertiary Care HospitalAnonymous TzvMOnNo ratings yet
- QH Nutrition Standards PDFDocument66 pagesQH Nutrition Standards PDFTydo WadyNo ratings yet
- PRC Case Form (or-DR Filled) - FinalDocument5 pagesPRC Case Form (or-DR Filled) - Finalredland1720005500No ratings yet
- Reteaua Eureko BucurestiDocument4 pagesReteaua Eureko BucurestiAna-Maria EneNo ratings yet
- Peritonitis Clinical Pathway PDFDocument4 pagesPeritonitis Clinical Pathway PDFIndah95No ratings yet
- Dental Clinic ServicesDocument3 pagesDental Clinic ServicesRoland NicolasNo ratings yet
- 3 The Health Care Delivery SystemDocument5 pages3 The Health Care Delivery SystemMikhaela Andree Mariano100% (1)
- Delirium: in The ClinicDocument16 pagesDelirium: in The Clinicmedal6No ratings yet
- Manila East Medical Center MEMC BLDG., Manila East Rd.,Taytay, 1920 Rizal, PhilippinesDocument2 pagesManila East Medical Center MEMC BLDG., Manila East Rd.,Taytay, 1920 Rizal, PhilippineshoneyleensorianoNo ratings yet
- An Introduction To Insulin TherapyDocument23 pagesAn Introduction To Insulin TherapyOrion JohnNo ratings yet
- Neha JohnDocument17 pagesNeha Johndeepika kushwah100% (1)
- As ISO 10993.4-2003 Biological Evaluation of Medical Devices Selection of Tests For Interactions With BloodDocument10 pagesAs ISO 10993.4-2003 Biological Evaluation of Medical Devices Selection of Tests For Interactions With BloodSAI Global - APACNo ratings yet
- Conceptual FrameworkDocument2 pagesConceptual FrameworkChristine Del Fierro Abran100% (1)
- PESSIDocument2 pagesPESSIFaria AslamNo ratings yet
- Form 1. Application For Travel and Accommodation Assistance - April 2019Document4 pagesForm 1. Application For Travel and Accommodation Assistance - April 2019chris tNo ratings yet
- Conference ProgrammeDocument24 pagesConference ProgrammeMaya FikriNo ratings yet
- Palliative Care For The Patient With Incurable Cancer or Advanced DiseaseDocument73 pagesPalliative Care For The Patient With Incurable Cancer or Advanced DiseaseArif HameedNo ratings yet
- ISQua Programme KL 2018 PDFDocument144 pagesISQua Programme KL 2018 PDFSuresh MikeNo ratings yet
- Care Bundles in Intensive CareDocument4 pagesCare Bundles in Intensive CareYashoda PereraNo ratings yet
- Arnold Palmer HospitalDocument1 pageArnold Palmer Hospitaldev26v8No ratings yet
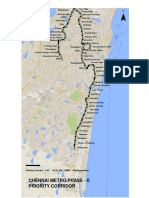
- Chennai Metro Phase - Ii Priority CorridorDocument1 pageChennai Metro Phase - Ii Priority CorridorAvinash SNo ratings yet
- Poster Presentation Nur 4242 KDocument1 pagePoster Presentation Nur 4242 Kapi-340245019No ratings yet