You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 01-09 2022 Pharm Chronic Care in Cardiology 2022 R4Document62 pages01-09 2022 Pharm Chronic Care in Cardiology 2022 R4Amira HelayelNo ratings yet
- Doze IECA - SartaniDocument2 pagesDoze IECA - SartaniAlexandraNo ratings yet
- 7189 Nitrosamine and Mutagenic Impurities Application GuideDocument89 pages7189 Nitrosamine and Mutagenic Impurities Application GuideMohd Firkhry Fadhly Abdul GhaniNo ratings yet
- Highlights of 1469 Nitrosamine ImpuritiesDocument28 pagesHighlights of 1469 Nitrosamine ImpuritiesWidiyantoNo ratings yet
- Journals-EURO-EURO2021007.The GDPR and Processing of Personal Data For Research Purposes What About Case LawDocument24 pagesJournals-EURO-EURO2021007.The GDPR and Processing of Personal Data For Research Purposes What About Case Law别康民No ratings yet
- SM - 113 - 0039.interest of Inertial Measurement Unit Tool in The Functional Evaluation of Ankle Evertor Muscles in Trail RunningDocument6 pagesSM - 113 - 0039.interest of Inertial Measurement Unit Tool in The Functional Evaluation of Ankle Evertor Muscles in Trail Running别康民No ratings yet
- PP9940255.Carbohydrate Storage and Mobilisation by The Culm of Wheat Between Heading and Grain Maturity The Relation To Sucrose Synthase and Sucrose-Phosphate SynthaseDocument17 pagesPP9940255.Carbohydrate Storage and Mobilisation by The Culm of Wheat Between Heading and Grain Maturity The Relation To Sucrose Synthase and Sucrose-Phosphate Synthase别康民No ratings yet
- 基于先进调制的高速可见光通信技术Document5 pages基于先进调制的高速可见光通信技术别康民No ratings yet
- Structures of (Beta) - GlycosidaDocument4 pagesStructures of (Beta) - Glycosida别康民No ratings yet
- Bespoke Library Docking For 5-HT Receptor Agonists With Antidepressant ActivityDocument36 pagesBespoke Library Docking For 5-HT Receptor Agonists With Antidepressant Activity别康民No ratings yet
- 1 s2.0 S0010218022003790 MainDocument17 pages1 s2.0 S0010218022003790 Main别康民No ratings yet
- Soil Carbon Sequestration by Root Exudates: Plant ScienceDocument9 pagesSoil Carbon Sequestration by Root Exudates: Plant Science别康民No ratings yet
- 1 s2.0 S1540748922002073 MainDocument10 pages1 s2.0 S1540748922002073 Main别康民No ratings yet
- 1 s2.0 S1540748922002668 MainDocument10 pages1 s2.0 S1540748922002668 Main别康民No ratings yet
- Photoexcited Nitroarenes For The Oxidative Cleavage of AlkenesDocument7 pagesPhotoexcited Nitroarenes For The Oxidative Cleavage of Alkenes别康民No ratings yet
- 1 s2.0 S1931312821005795 MainDocument19 pages1 s2.0 S1931312821005795 Main别康民No ratings yet
- Bishop-Davy1985 Article DensityAndTheCommitmentOfApicaDocument6 pagesBishop-Davy1985 Article DensityAndTheCommitmentOfApica别康民No ratings yet
- Receptor-Like Protein Kinase Bak1 Promotes K Uptake by Regulating H - Atpase Aha2 Under Low Potassium StressDocument53 pagesReceptor-Like Protein Kinase Bak1 Promotes K Uptake by Regulating H - Atpase Aha2 Under Low Potassium Stress别康民No ratings yet
- Engineering Apomixis: Clonal Seeds Approaching The Fields: Annual Review of Plant BiologyDocument28 pagesEngineering Apomixis: Clonal Seeds Approaching The Fields: Annual Review of Plant Biology别康民No ratings yet
- Homogenizing Silicon Domains in Sio Anode During Cycling and Enhancing Battery Performance Via Magnesium DopingDocument13 pagesHomogenizing Silicon Domains in Sio Anode During Cycling and Enhancing Battery Performance Via Magnesium Doping别康民No ratings yet
- D Vaccine EfficacyDocument11 pagesD Vaccine Efficacy别康民No ratings yet
- Study On Friction Reduction and Wear Resistance of Surface Micro Texture of YG8 Ti6Al4V Friction PairDocument15 pagesStudy On Friction Reduction and Wear Resistance of Surface Micro Texture of YG8 Ti6Al4V Friction Pair别康民No ratings yet
- Psidium Guajava Flavonoids Prevent NLRP3Document15 pagesPsidium Guajava Flavonoids Prevent NLRP3别康民No ratings yet
- A Study About One Kind of Two Dimensional Integral Equation of Volterra Type With Two Interior Singular LinesDocument9 pagesA Study About One Kind of Two Dimensional Integral Equation of Volterra Type With Two Interior Singular Lines别康民No ratings yet
- Wartime Women Rape: A Means of Moral Attack and Emasculation in Lynn Nottage's RuinedDocument8 pagesWartime Women Rape: A Means of Moral Attack and Emasculation in Lynn Nottage's Ruined别康民No ratings yet
- Rem Pel 1978Document19 pagesRem Pel 1978别康民No ratings yet
- The Historical Slave Trade and Firm Access To Finance in AfricaDocument33 pagesThe Historical Slave Trade and Firm Access To Finance in Africa别康民No ratings yet
- Wang 2018Document57 pagesWang 2018别康民No ratings yet
- Geographical Indications and Innovation, What Is The Connection?Document34 pagesGeographical Indications and Innovation, What Is The Connection?别康民No ratings yet
- MCL Policy 2015Document89 pagesMCL Policy 2015别康民No ratings yet
- Sun 2016Document10 pagesSun 2016别康民No ratings yet
- Emotional Ai: Andrew McstayDocument12 pagesEmotional Ai: Andrew Mcstay别康民No ratings yet
- Multiple Lot in One Foup (Mlif) Control and Management in The 300Mm FabDocument4 pagesMultiple Lot in One Foup (Mlif) Control and Management in The 300Mm Fab别康民No ratings yet
- ACE Inhibitors Vs ARBs Is One Class Better For HeaDocument7 pagesACE Inhibitors Vs ARBs Is One Class Better For HeaAfisya sawkiNo ratings yet
- SacubitrilValsartan (Entresto) For Heart FailureDocument2 pagesSacubitrilValsartan (Entresto) For Heart FailureWatchara TansiriNo ratings yet
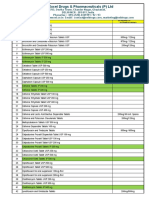
- VXL-List of Pharma Products (Domestic and Export)Document10 pagesVXL-List of Pharma Products (Domestic and Export)Singh PushpanjaliNo ratings yet
- Nitrosamines in Pharmaceuticals Toxicity Risk Analysis Chemistry and Test Methods - Kiran KotaDocument11 pagesNitrosamines in Pharmaceuticals Toxicity Risk Analysis Chemistry and Test Methods - Kiran Kotakiran100% (1)
- Coversam 4mg/5mg Tablets Coversam 4mg/10mg Tablets Coversam 8mg/5mg Tablets Coversam 8mg/10mg TabletsDocument2 pagesCoversam 4mg/5mg Tablets Coversam 4mg/10mg Tablets Coversam 8mg/5mg Tablets Coversam 8mg/10mg TabletsRaheel Neo AhmadNo ratings yet
- 1.prezentacija Seminarski Marketing U FarmacijiDocument16 pages1.prezentacija Seminarski Marketing U FarmacijimajamunitlakNo ratings yet
- Valsartan SynthesisDocument5 pagesValsartan SynthesisKartar ChavhanNo ratings yet
- Co DiovanDocument8 pagesCo DiovanPeter Rey Tanio TeopeNo ratings yet
- D Jothiewari Et. Al.. (UV)Document5 pagesD Jothiewari Et. Al.. (UV)EVELYN SOLANHS ACERO RODRIGUEZNo ratings yet
- Valsartan in The Treatment of Hypertension: OriginalDocument4 pagesValsartan in The Treatment of Hypertension: Originaldini hanifaNo ratings yet
- Matsushita 2010Document7 pagesMatsushita 2010Arankesh MNo ratings yet
- Angiotensin Receptor Blockers (O)Document26 pagesAngiotensin Receptor Blockers (O)farmasi_hmNo ratings yet
- ValsartanDocument3 pagesValsartanapi-3797941100% (1)
- Pharmacology Questions CardiacDocument5 pagesPharmacology Questions CardiacAmanda SimpsonNo ratings yet
- BlokatensDocument3 pagesBlokatensDarkmatter DarkmatterrNo ratings yet
- S1.1 Ria Bandiara - Role Managemen Hypertension PKB 2019Document29 pagesS1.1 Ria Bandiara - Role Managemen Hypertension PKB 2019siputleletNo ratings yet
- Hipertensi DM PDFDocument32 pagesHipertensi DM PDFRian HutabaratNo ratings yet
- Zelisar Marketing Plan For Spain: Novartis Masterminds ChallengeDocument14 pagesZelisar Marketing Plan For Spain: Novartis Masterminds Challengealdusc3No ratings yet
- List Obat TambahanDocument42 pagesList Obat TambahanImroatus SholihahNo ratings yet
- Draft PDFDocument166 pagesDraft PDFashwaq000111No ratings yet
- Exforge Juga NihDocument10 pagesExforge Juga Nihani rahayuNo ratings yet
- Intertek Fact Sheet Nitrosamine Impurity Analysis ARB MedicinesDocument1 pageIntertek Fact Sheet Nitrosamine Impurity Analysis ARB MedicinesROBINNo ratings yet
- The Different Therapeutic Choices With Arbs. Which One To Give? When? Why?Document28 pagesThe Different Therapeutic Choices With Arbs. Which One To Give? When? Why?Rajeev GuptaNo ratings yet
- Entresto Uses, Dosage, Side Effects & WarningsDocument6 pagesEntresto Uses, Dosage, Side Effects & WarningspatgarettNo ratings yet
- European J of Heart Fail - 2021 - Greene - Another Reason To Embrace Quadruple Medical Therapy For Heart FailureDocument4 pagesEuropean J of Heart Fail - 2021 - Greene - Another Reason To Embrace Quadruple Medical Therapy For Heart FailureSrinivas PingaliNo ratings yet
- Amlodipine Valsartan 2Document8 pagesAmlodipine Valsartan 2Anggun Nurul FitriaNo ratings yet