You might also like
- SmartForm - Invoice TutorialDocument17 pagesSmartForm - Invoice TutorialShelly McRay100% (5)
- Member StiffnessDocument22 pagesMember Stiffnessapi-451702331No ratings yet
- Jyotsna FinalDocument59 pagesJyotsna FinalSheena GandhiNo ratings yet
- Who 2010Document18 pagesWho 2010ananya Dan (anya)No ratings yet
- International Journal For Equity in HealthDocument10 pagesInternational Journal For Equity in HealthNelmarcioNo ratings yet
- Getting India's Health Care System Out of The ICUDocument2 pagesGetting India's Health Care System Out of The ICUPulokesh GhoshNo ratings yet
- CSIS Policy Brief Reforming Sustainable Healthcare System Lesson Learned From Three Countries in ASEANDocument17 pagesCSIS Policy Brief Reforming Sustainable Healthcare System Lesson Learned From Three Countries in ASEANBersama Budi Kembali BerbaktiNo ratings yet
- NCSC AssessmentDocument4 pagesNCSC AssessmentSushila KispottaNo ratings yet
- P1 PDFDocument10 pagesP1 PDFMridul PantNo ratings yet
- "We Are Called The Et Cetera": Experiences of The Poor With Health Financing Reforms That Target Them in KenyaDocument14 pages"We Are Called The Et Cetera": Experiences of The Poor With Health Financing Reforms That Target Them in KenyaASHUTOSH OJHANo ratings yet
- Health and Economic Development: Linkage and ImpactDocument21 pagesHealth and Economic Development: Linkage and ImpactDora SimmonsNo ratings yet
- Review Jurnal Pembiayaan Kesehatan 2Document5 pagesReview Jurnal Pembiayaan Kesehatan 2SUCI PERMATANo ratings yet
- Health CareDocument203 pagesHealth CareNiro ThakurNo ratings yet
- Health-Fi Nancing Reforms in Southeast AsiaDocument12 pagesHealth-Fi Nancing Reforms in Southeast AsiaKutu KupretNo ratings yet
- Unsatisfaction Pacient in Healthy Industrial in Indonesia: Ahmad Zafrullah Tayibnapis, Lucia E. WuryaningsihDocument9 pagesUnsatisfaction Pacient in Healthy Industrial in Indonesia: Ahmad Zafrullah Tayibnapis, Lucia E. WuryaningsihtheijesNo ratings yet
- Fixing India's Healthcare System - Carnegie Endowment For International PeaceDocument3 pagesFixing India's Healthcare System - Carnegie Endowment For International PeaceMohammad UzairNo ratings yet
- Health Financing Reform in Uganda: How Equitable Is The Proposed National Health Insurance Scheme?Document8 pagesHealth Financing Reform in Uganda: How Equitable Is The Proposed National Health Insurance Scheme?Byaruhanga EmmanuelNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Latihan NormalisasiDocument3 pagesLatihan NormalisasiFadil0% (1)
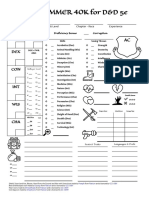
- WARHAMMER 40K For D&D 5e: Character Name Class & Level Chapter - Race ExperienceDocument1 pageWARHAMMER 40K For D&D 5e: Character Name Class & Level Chapter - Race ExperienceJacob CooperNo ratings yet
- Fiber Cable Preparation, Splicing, and Termination InstructionsDocument8 pagesFiber Cable Preparation, Splicing, and Termination InstructionsHunaAdjaganNo ratings yet
- Venturi-Based Two-Layer Microfluidic Pumping SystemDocument3 pagesVenturi-Based Two-Layer Microfluidic Pumping SystemManu Ele100% (1)
- Marrin - CIA Kent School and University-2000Document3 pagesMarrin - CIA Kent School and University-2000Stephen MarrinNo ratings yet
- ENGL 0101 Graded Quiz Unit 6Document3 pagesENGL 0101 Graded Quiz Unit 6Mark AntonyNo ratings yet
- Comparison and ContrastDocument9 pagesComparison and ContrastCrash BandicootNo ratings yet
- Blood SpatterDocument13 pagesBlood SpatterGabriel Stossel (2020)No ratings yet
- Scientific Explanation of GITADocument29 pagesScientific Explanation of GITARamakrishna ReddyNo ratings yet
- Me Law Me SyllabiDocument12 pagesMe Law Me SyllabiVon A. DamirezNo ratings yet
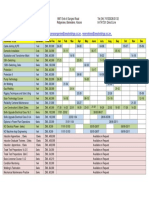
- Technical Training Calendar 20220122Document1 pageTechnical Training Calendar 20220122Lawson Shumirai Sango100% (1)
- Magallanes National Vocational High SchoolDocument2 pagesMagallanes National Vocational High SchoolJohn Arol De LeonNo ratings yet
- Mathcad - Foster 24-Hour HyetogDocument12 pagesMathcad - Foster 24-Hour Hyetogelgheryb_choukriNo ratings yet
- Attacker "Math" 101: Professor Dai Zovi Institute For The Advancement of Memory CorruptionDocument47 pagesAttacker "Math" 101: Professor Dai Zovi Institute For The Advancement of Memory CorruptionnewvpupkinNo ratings yet
- CH99225A - A and E - Structural - CH99225 - NSD Template - Ring (469745) (CH99225A - A and E - Structural - 06.01.15 - Pass)Document34 pagesCH99225A - A and E - Structural - CH99225 - NSD Template - Ring (469745) (CH99225A - A and E - Structural - 06.01.15 - Pass)John Neil MitraNo ratings yet
- Question 13Document4 pagesQuestion 13HotSpireNo ratings yet
- Advanced English 3 (I)Document7 pagesAdvanced English 3 (I)Anonymous XETUXbV1No ratings yet
- Hypothesis Tests About The Mean and ProportionDocument109 pagesHypothesis Tests About The Mean and Proportion03435013877100% (1)
- CodeDocument95 pagesCodeVijji VijayNo ratings yet
- Analysis Process Designer (APD) Part23 - 12 PDFDocument19 pagesAnalysis Process Designer (APD) Part23 - 12 PDFAshok ReddyNo ratings yet
- Jira Software Server 070-131015Document283 pagesJira Software Server 070-131015Srikant GummadiNo ratings yet
- Tedtalks: Malcolm Gladwell: The Strange Tale of The Norden BombsightDocument9 pagesTedtalks: Malcolm Gladwell: The Strange Tale of The Norden BombsightalibrownNo ratings yet
- Step 1 LibraryDocument20 pagesStep 1 LibraryLaith الكويس Omar ANo ratings yet
- Power of Imagination in SadhanaDocument7 pagesPower of Imagination in SadhanaSwami VedatitanandaNo ratings yet
- Amazon Has Just Shown Off The Most Advanced Technology StoreDocument3 pagesAmazon Has Just Shown Off The Most Advanced Technology StoreEmanuel VasconcelosNo ratings yet
- Imelda EsmaeiliDocument2 pagesImelda Esmaeiliapi-285453553No ratings yet
- Monograph Professional Business Communication PCT 610Document88 pagesMonograph Professional Business Communication PCT 610ShreyaSinglaNo ratings yet