You might also like
- Basic Occupational Health Services A Complete Guide - 2020 EditionFrom EverandBasic Occupational Health Services A Complete Guide - 2020 EditionNo ratings yet
- Food Safety PDFDocument11 pagesFood Safety PDFMaria AnnieskaNo ratings yet
- Proprietor food safetyDocument3 pagesProprietor food safetyKenneth Alsola100% (1)
- Unit II Food Safety and Hygiene SanitationDocument25 pagesUnit II Food Safety and Hygiene SanitationShaira Arrocena SagsagatNo ratings yet
- Lesson 4 WorksheetDocument16 pagesLesson 4 WorksheetAmy Evans0% (1)
- Institutional Food ManagementDocument10 pagesInstitutional Food ManagementSurya NivruthaNo ratings yet
- Food Poisoning: - Also Known As Foodborne Illness - Is Any Illness That Results FromDocument24 pagesFood Poisoning: - Also Known As Foodborne Illness - Is Any Illness That Results FromTheodiffer Digal TemblorNo ratings yet
- Employee Food Safety Training RecordDocument1 pageEmployee Food Safety Training RecordSulaiman AhmatNo ratings yet
- Food Fortification NewDocument16 pagesFood Fortification NewKathryn Faith MalabagNo ratings yet
- Basic Hygiene PracticeDocument24 pagesBasic Hygiene PracticeVijin RajNo ratings yet
- Food Safety Using HACCPDocument8 pagesFood Safety Using HACCPYant RUma ButarNo ratings yet
- Principles of Safety Hygiene & Sanitation (SANGENEDocument42 pagesPrinciples of Safety Hygiene & Sanitation (SANGENEgregNo ratings yet
- The Food and Beverage DepartmentDocument40 pagesThe Food and Beverage DepartmentChristian CandareNo ratings yet
- Food safety regulations guide quality assuranceDocument6 pagesFood safety regulations guide quality assuranceabdul RahmanNo ratings yet
- Registration FormDocument2 pagesRegistration FormAlex Maverick WhittakerNo ratings yet
- Veg Diet Plan PDFDocument3 pagesVeg Diet Plan PDFplus100yearsNo ratings yet
- Assignment (The Menu)Document1 pageAssignment (The Menu)Nurliyana Athirah FakharulraziNo ratings yet
- HACCP Plan Fruit Salad PDFDocument22 pagesHACCP Plan Fruit Salad PDFAliNo ratings yet
- Assessment of Nutritional SituationDocument24 pagesAssessment of Nutritional SituationMawasumi Ayu Andini0% (1)
- Food Hygine Final TypingDocument53 pagesFood Hygine Final TypingSally Salina Farah50% (2)
- (World Health Organization) FAO WHO Guidance To Go HACCPDocument84 pages(World Health Organization) FAO WHO Guidance To Go HACCPNoor Wahyu Sugeng RNo ratings yet
- Cooksafe House RulesDocument19 pagesCooksafe House RulesMUHAMMAD SUHAIB TAHIRNo ratings yet
- SushiDocument9 pagesSushishankarzoneNo ratings yet
- Food Allergies and Intolerances ExplainedDocument94 pagesFood Allergies and Intolerances ExplainedSrikanth ReddyNo ratings yet
- Promoting Healthy Aging, Independence and Quality of LifeDocument15 pagesPromoting Healthy Aging, Independence and Quality of LifeEvelyn MedinaNo ratings yet
- QP THC Q3006 Multi Cuisine CookDocument71 pagesQP THC Q3006 Multi Cuisine Cooknayra khanNo ratings yet
- HACCP and Food Safety Principles ExplainedDocument13 pagesHACCP and Food Safety Principles ExplainedNorma Panares100% (1)
- Sanitary Food Handling in Foodservice: About This ChapterDocument24 pagesSanitary Food Handling in Foodservice: About This ChapterRaul TejedaNo ratings yet
- Food Safety and HygieneDocument32 pagesFood Safety and HygieneJulia El SamraNo ratings yet
- RSPH Level 4 Award in Haccp Management For Food ManufacturingDocument19 pagesRSPH Level 4 Award in Haccp Management For Food ManufacturingHema HemaNo ratings yet
- National Policy On Food and Nutrition 2016 PDFDocument50 pagesNational Policy On Food and Nutrition 2016 PDFTemiNo ratings yet
- Training Report On Regenerative Health and Nutrition For Nutriion OfficersDocument7 pagesTraining Report On Regenerative Health and Nutrition For Nutriion OfficersibnmamaniNo ratings yet
- BNF Food Poisoning Tcm4-662860Document23 pagesBNF Food Poisoning Tcm4-662860clinical_pathologyNo ratings yet
- Infection Control in NurseryDocument5 pagesInfection Control in Nurserysandeepv08No ratings yet
- I. Introduction To Food ProductionDocument50 pagesI. Introduction To Food ProductionMa.Lourdes Corpuz100% (1)
- Nutritional AssessmentDocument8 pagesNutritional AssessmentOutour KhNo ratings yet
- Expo Job Descrip 1998Document2 pagesExpo Job Descrip 1998Lancemachang EugenioNo ratings yet
- Food Hygiene Practices: Hazard Analysis (HA) - HA Is Based On Five Principles, Detailed at Annex A To This ChapterDocument88 pagesFood Hygiene Practices: Hazard Analysis (HA) - HA Is Based On Five Principles, Detailed at Annex A To This ChapterKousik PaikNo ratings yet
- Allergens Slides Brown 031617Document16 pagesAllergens Slides Brown 031617almutazimNo ratings yet
- Food PoisoningDocument42 pagesFood Poisoningalif67% (3)
- Unit 6-Nutrition and HydrationDocument109 pagesUnit 6-Nutrition and Hydration1sylvialee100% (2)
- Food Handler GuidelinesDocument156 pagesFood Handler GuidelinesAhmed KamalNo ratings yet
- MIDC Unit1, 4Document22 pagesMIDC Unit1, 401 Rabia AhmedNo ratings yet
- Food Safety Management ProceeduresDocument4 pagesFood Safety Management ProceeduresRulment DardaneiNo ratings yet
- g7 - Record 11 - Initial Staff Food Safety Information DeclarationDocument1 pageg7 - Record 11 - Initial Staff Food Safety Information DeclarationRyzal9marchNo ratings yet
- Washing Fruits and VegetablesDocument2 pagesWashing Fruits and VegetablesSaravana KumarNo ratings yet
- Occupational Health and Safety Lesson PlanDocument3 pagesOccupational Health and Safety Lesson PlanDonna Marie ArcangelNo ratings yet
- Food Processing1Document19 pagesFood Processing1daabgchiNo ratings yet
- Module 1 Trainer Manual PDFDocument26 pagesModule 1 Trainer Manual PDFSanath KamilaNo ratings yet
- Classification of Fs System 1Document26 pagesClassification of Fs System 1Prasanna SpideyNo ratings yet
- Chapter 2 - THE SAFE FOOD HANDLER PDFDocument83 pagesChapter 2 - THE SAFE FOOD HANDLER PDFGeraldine Roque ApiadoNo ratings yet
- How Better Outbreak Investigations Can Make The Food Supply SaferDocument64 pagesHow Better Outbreak Investigations Can Make The Food Supply SaferNational Press FoundationNo ratings yet
- Enteral and Parenteral Nutrition SeminarDocument20 pagesEnteral and Parenteral Nutrition SeminarAmin AksherNo ratings yet
- Standard Port Health Inspection GuidelinesDocument11 pagesStandard Port Health Inspection GuidelinesWayan PandeNo ratings yet
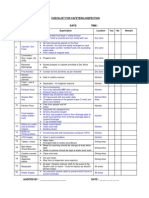
- Microsoft Word - Checklist For Cafeteria Inspection - LatestDocument1 pageMicrosoft Word - Checklist For Cafeteria Inspection - LatestAyong EntilyNo ratings yet
- Kitchen Safety Report on Hazards, Risks and RegulationsDocument27 pagesKitchen Safety Report on Hazards, Risks and RegulationsJay Lord Santos SalvadorNo ratings yet
- 13 - Food Hygiene TemplatesDocument17 pages13 - Food Hygiene TemplatessurajNo ratings yet
- Catering PatientsDocument32 pagesCatering PatientsBrian Shanny100% (1)
- 564 140 1011Document1 page564 140 1011morneNo ratings yet
- 564 320 10Document1 page564 320 10morneNo ratings yet
- Codewest 510 Pre-Course Study Guide May 2015Document76 pagesCodewest 510 Pre-Course Study Guide May 2015oluninjaa100% (4)
- CKRC API 510 WORKBOOK MODULE 1 Rev 1Document7 pagesCKRC API 510 WORKBOOK MODULE 1 Rev 1morneNo ratings yet
- Codewest 510 Pre-Course Study Guide May 2015Document76 pagesCodewest 510 Pre-Course Study Guide May 2015oluninjaa100% (4)
- B BBEE AffidavitDocument1 pageB BBEE AffidavitRhyno HeydenrychNo ratings yet
- Steval Engineering: A213-MMC-SVE-RFI-001Document1 pageSteval Engineering: A213-MMC-SVE-RFI-001morneNo ratings yet
- Health and Safety Officer CompetenciesDocument24 pagesHealth and Safety Officer CompetenciesAminur HaqiemNo ratings yet
- Baker & Confectioner: Competency Based CurriculumDocument31 pagesBaker & Confectioner: Competency Based CurriculumEyock PierreNo ratings yet
- HSE Training MatrixDocument1 pageHSE Training MatrixAbdus SamadNo ratings yet
- 4600 Plum Eye Wash 112015 UKDocument7 pages4600 Plum Eye Wash 112015 UKArdXkillerNo ratings yet
- Staff Induction Checklist: Social Services and HousingDocument14 pagesStaff Induction Checklist: Social Services and HousingLoveNo ratings yet
- MIT Pressure Vessel ProceduresDocument9 pagesMIT Pressure Vessel ProceduresMonica WijayaNo ratings yet
- SMR-3500LV TDSDocument1 pageSMR-3500LV TDSTrevor MarronNo ratings yet
- QuestionsDocument45 pagesQuestionsA.A M.A.RNo ratings yet
- Carbon TetrachlorideDocument5 pagesCarbon Tetrachloridesummi64No ratings yet
- Module TwoDocument97 pagesModule TwoJeh UbaldoNo ratings yet
- Remigio Vs NLRCDocument12 pagesRemigio Vs NLRCCali AustriaNo ratings yet
- Health and Safety in Relation To The Use of ICT SystemsDocument2 pagesHealth and Safety in Relation To The Use of ICT SystemsjazfirouziNo ratings yet
- G.R. No. 187950 CRISTINA BARSOLO, Petitioner, Social Security System, Respondent. Decision Leonen, J.Document25 pagesG.R. No. 187950 CRISTINA BARSOLO, Petitioner, Social Security System, Respondent. Decision Leonen, J.Moachi SianenNo ratings yet
- 07Document1 page07lakshi fernandoNo ratings yet
- l08 - Doohickeys Report 2Document14 pagesl08 - Doohickeys Report 2api-461706989No ratings yet
- AHB Hong KongDocument46 pagesAHB Hong KongPraveen SankaranNo ratings yet
- Operation Manual 1760xl-OmDocument116 pagesOperation Manual 1760xl-Omrce.ramNo ratings yet
- Safety Data Sheet: 1: IdentificationDocument10 pagesSafety Data Sheet: 1: IdentificationManuel MoriveraNo ratings yet
- MSDS Sulzer Metco 4198Document10 pagesMSDS Sulzer Metco 4198candraNo ratings yet
- Housekeeping NC III CBCDocument84 pagesHousekeeping NC III CBCBlessy Alina100% (1)
- HIRAC Work at HeightDocument7 pagesHIRAC Work at HeightMitchRappNo ratings yet
- ABS Material Safety Data SheetDocument8 pagesABS Material Safety Data SheetEduardo GarzaNo ratings yet
- Tyre storage and fire safety guidelinesDocument78 pagesTyre storage and fire safety guidelineslkulacogluNo ratings yet
- Twi Brochure 2013Document86 pagesTwi Brochure 2013balusandeep20100% (1)
- JCI REACH RoHS Awareness Presentation - 2Document6 pagesJCI REACH RoHS Awareness Presentation - 2Diptarghya KunduNo ratings yet
- DLL Cookery Classroom ObservationDocument4 pagesDLL Cookery Classroom ObservationMICHELLE RAFAELNo ratings yet
- Almeria - Matanga - Look - Talustusan - Padre - Inocentes - Biliran - BachaoDocument6 pagesAlmeria - Matanga - Look - Talustusan - Padre - Inocentes - Biliran - BachaoKaye TagnipesNo ratings yet
- Surtec 650V MsdsDocument7 pagesSurtec 650V MsdsjkljNo ratings yet
- ARTICULO Telecomunicaciones 02-09-2020IIDocument15 pagesARTICULO Telecomunicaciones 02-09-2020IISEBASTIAN LOPEZ RAMIREZ0% (1)
- C&D MSDSDocument10 pagesC&D MSDSDhiraj KapoorNo ratings yet