You might also like
- Breast Cancer: Melatonin Helps to: Prevent Cancer, Avoid Drug Resistance, Stop MetastasisFrom EverandBreast Cancer: Melatonin Helps to: Prevent Cancer, Avoid Drug Resistance, Stop MetastasisNo ratings yet
- Menopause Symptoms, Causes, and Treatments ExplainedDocument35 pagesMenopause Symptoms, Causes, and Treatments ExplainedCALVO, JUAN BERNARDONo ratings yet
- The Journey of Pregnancy: Conception – Pregnancy – Delivery – AftercareFrom EverandThe Journey of Pregnancy: Conception – Pregnancy – Delivery – AftercareNo ratings yet
- ChronopharmacokineticsDocument38 pagesChronopharmacokineticsvaibhav5414No ratings yet
- Heavy Menstrual BleedingDocument29 pagesHeavy Menstrual BleedingsanjupainNo ratings yet
- Physiology of PregnancyDocument31 pagesPhysiology of PregnancyPutra Mahautama100% (1)
- Answers BiostatsDocument2 pagesAnswers BiostatsNitesh67% (3)
- Intrahepatic Cholestasis of PregnancyDocument19 pagesIntrahepatic Cholestasis of PregnancyAlexander Vasquez TorresNo ratings yet
- Complementary and Alternative Approach For Pain Management in LabourDocument9 pagesComplementary and Alternative Approach For Pain Management in LabourPujianti LestarinaNo ratings yet
- NSG Education SeminarDocument27 pagesNSG Education SeminarBHUKYA USHARANINo ratings yet
- Chronopharmacology 120325134521 Phpapp02Document35 pagesChronopharmacology 120325134521 Phpapp02Selva Rathinam0% (1)
- Approach To The Patient With An Adnexal Mass - UpToDateDocument31 pagesApproach To The Patient With An Adnexal Mass - UpToDateRamackNo ratings yet
- MENSTRUAL CYCLE GUIDEDocument77 pagesMENSTRUAL CYCLE GUIDEAlivia SoerayaNo ratings yet
- 1.113.medication Administration TimingDocument14 pages1.113.medication Administration TimingSophiaNo ratings yet
- Oral and Parenteral Iron Preparations in PregnancyDocument45 pagesOral and Parenteral Iron Preparations in PregnancyArun George100% (3)
- Contraception: DR Husni SamarahDocument15 pagesContraception: DR Husni Samarahpal_pal_palNo ratings yet
- The Physiology of Human Sexual Act (Final)Document16 pagesThe Physiology of Human Sexual Act (Final)NatnaelNo ratings yet
- SLE-combined 2 ArshadDocument71 pagesSLE-combined 2 ArshadarshadsyahaliNo ratings yet
- Infections of Female Genital TractDocument67 pagesInfections of Female Genital TractSana AftabNo ratings yet
- Traditional Systems of Medicines. F19 FinaldocxDocument8 pagesTraditional Systems of Medicines. F19 FinaldocxAroob FaisalNo ratings yet
- Peripheral Nervous System: Structure, Functions of Cranial Nerves and Autonomic Nervous SystemDocument52 pagesPeripheral Nervous System: Structure, Functions of Cranial Nerves and Autonomic Nervous SystemRizki PerdanaNo ratings yet
- Thyroid Disease in PregnancyDocument36 pagesThyroid Disease in Pregnancypeni_dwiNo ratings yet
- Differential Diagnosis of The Adnexal Mass 2020Document38 pagesDifferential Diagnosis of The Adnexal Mass 2020Sonia MVNo ratings yet
- 204-02 Human Anatomy Physiology II - LECTDocument9 pages204-02 Human Anatomy Physiology II - LECTGagandeep SinghNo ratings yet
- Biochemical Investigation in PregDocument28 pagesBiochemical Investigation in PregRana VandanaNo ratings yet
- HMBDocument41 pagesHMBakmal3501No ratings yet
- Diabeties NewDocument54 pagesDiabeties NewDipti SharmaNo ratings yet
- Hormonal Contraceptive MethodsDocument70 pagesHormonal Contraceptive MethodsMaldini NyachNo ratings yet
- Anesthetic Efficacy of Clove Oil and Its Impact On Hematological and Biochemical Changes in Channa Striatus (Bloch, 1793)Document9 pagesAnesthetic Efficacy of Clove Oil and Its Impact On Hematological and Biochemical Changes in Channa Striatus (Bloch, 1793)researchinbiologyNo ratings yet
- Reproductive EndocrinologyDocument18 pagesReproductive EndocrinologyAnonymous hkWIKjoXFVNo ratings yet
- Infertility 1Document2 pagesInfertility 1Mikhaela Andree MarianoNo ratings yet
- Impact of Menopause On Quality of Life Among Indian WomenDocument16 pagesImpact of Menopause On Quality of Life Among Indian WomenGlobal Research and Development ServicesNo ratings yet
- Management of Infertility: Presented By: Dr. Sheetal M Savaliya Guide: Dr. Anil P Singh Co-Guide: Dr. Shailesh MundhavaDocument37 pagesManagement of Infertility: Presented By: Dr. Sheetal M Savaliya Guide: Dr. Anil P Singh Co-Guide: Dr. Shailesh MundhavaBhawna JoshiNo ratings yet
- Benign Ovarian TumorsDocument38 pagesBenign Ovarian Tumorssimi yNo ratings yet
- PsoriasisDocument4 pagesPsoriasisLau ColastreNo ratings yet
- IV Therapy Guide: Proper Administration and Potential ComplicationsDocument10 pagesIV Therapy Guide: Proper Administration and Potential ComplicationsacqueNo ratings yet
- Infertility IDocument36 pagesInfertility Idr_asaleh100% (1)
- Water Birth Definition & BenefitsDocument4 pagesWater Birth Definition & BenefitsindahNo ratings yet
- Female InfertilityDocument4 pagesFemale InfertilityAmar M AradhyaNo ratings yet
- SyphilisDocument22 pagesSyphilisKishor K AdhikariNo ratings yet
- Understanding Homoeopathy for PCOSDocument14 pagesUnderstanding Homoeopathy for PCOSHardikNo ratings yet
- The Artificial Pancreas How Will This Benefit Patiens With DIabetesDocument3 pagesThe Artificial Pancreas How Will This Benefit Patiens With DIabetesRebeca UrseNo ratings yet
- Rational Drug Prescribing Training CourseDocument78 pagesRational Drug Prescribing Training CourseAhmadu Shehu MohammedNo ratings yet
- IMLE Lecture on Obstetrics and Gynecology AnomaliesDocument69 pagesIMLE Lecture on Obstetrics and Gynecology AnomaliesTarek TarekNo ratings yet
- Dr Kihara's Guide to MenopauseDocument12 pagesDr Kihara's Guide to MenopauseAnonymous HHhuUgK0% (1)
- Menstrual DisordersDocument8 pagesMenstrual DisordersBangkit Pank BuminataNo ratings yet
- Vaginitis Case StudyDocument3 pagesVaginitis Case StudyYunEr Ong50% (2)
- HepatitisDocument3 pagesHepatitisElieth ConcepciónNo ratings yet
- Breastfeeding CounsellingDocument30 pagesBreastfeeding CounsellingHadeer Mahmoud AbuslimaNo ratings yet
- Hormonal ContraceptionDocument48 pagesHormonal ContraceptionO'Mark AndrewsNo ratings yet
- Nonpharmacologic Approaches To Management of Labor PainDocument32 pagesNonpharmacologic Approaches To Management of Labor PainFelipe DrummondNo ratings yet
- An AntipsychoticDocument4 pagesAn AntipsychoticJoMa TuazonNo ratings yet
- Menorrhagia (Heavy Menstrual Bleeding)Document55 pagesMenorrhagia (Heavy Menstrual Bleeding)Aizi DwimeilaNo ratings yet
- ARTICLE - 3 A Conceptual Study of Upavishtaka With Special Reference To IntrauterineDocument5 pagesARTICLE - 3 A Conceptual Study of Upavishtaka With Special Reference To IntrauterineKalpanaNo ratings yet
- 9fetal Well Being in PregnancyDocument10 pages9fetal Well Being in PregnancyuouoNo ratings yet
- Parts A and B Should Be Answered in Separate Answer Books. All Questions Carry Equal MarksDocument13 pagesParts A and B Should Be Answered in Separate Answer Books. All Questions Carry Equal MarksjishnuchandNo ratings yet
- Seminar On InfertilityDocument17 pagesSeminar On InfertilityN vineethaNo ratings yet
- Research On Mental HealthDocument21 pagesResearch On Mental HealthVaishnavi Priya JhaNo ratings yet
- Basics of Pharmacoeconomics and Outcomes ResearchDocument48 pagesBasics of Pharmacoeconomics and Outcomes ResearchArvind NagNo ratings yet
- MEDICAL INFO: CANCER PREVENTION TIPSDocument2 pagesMEDICAL INFO: CANCER PREVENTION TIPScmmc_3No ratings yet
- Titan InvoiceDocument1 pageTitan Invoiceiamdhanush017No ratings yet
- Mutual FundDocument2 pagesMutual Fundkum_praNo ratings yet
- PRESSURE VESSEL Handbook - Eugene F. Megyesy 12th 2001Document501 pagesPRESSURE VESSEL Handbook - Eugene F. Megyesy 12th 2001vamcodong71% (7)
- Exam Unit 1 Out and About 1º BachilleratoDocument5 pagesExam Unit 1 Out and About 1º Bachilleratolisikratis1980No ratings yet
- S-H Polarimeter Polartronic-532 Eng - 062015 PDFDocument2 pagesS-H Polarimeter Polartronic-532 Eng - 062015 PDFSuresh KumarNo ratings yet
- Overview of Research ProcessDocument31 pagesOverview of Research Processprema balusamyNo ratings yet
- Kütahya between the Lines: Uncovering Historical Insights from Post-Medieval CeramicsDocument24 pagesKütahya between the Lines: Uncovering Historical Insights from Post-Medieval Ceramicslatinist1No ratings yet
- 2019 Indonesia Salary GuideDocument32 pages2019 Indonesia Salary Guideiman100% (1)
- Lab Practice # 01 An Introduction To MatlabDocument10 pagesLab Practice # 01 An Introduction To MatlabGhulam Abbas LashariNo ratings yet
- Allison WallaceDocument3 pagesAllison WallaceOskar KarvajalNo ratings yet
- Articulos 2022-2Document11 pagesArticulos 2022-2Nilser Enrique Valle HernandezNo ratings yet
- Labconco-3905503 Rev e Purifier Hepa Filtered and Class I Filtered Enclosures User ManualDocument77 pagesLabconco-3905503 Rev e Purifier Hepa Filtered and Class I Filtered Enclosures User ManualCalixto GrajalesNo ratings yet
- Albert Einstein - Wikipedia, The Free EncyclopediaDocument34 pagesAlbert Einstein - Wikipedia, The Free EncyclopediaalhanunNo ratings yet
- IruvarDocument5 pagesIruvarKarthikeya KaredlaNo ratings yet
- PTR01 21050 90inst PDFDocument40 pagesPTR01 21050 90inst PDFЯн ПавловецNo ratings yet
- 6.1.2 The Solar SystemDocument4 pages6.1.2 The Solar System205 NursyazliyanaNo ratings yet
- Junguian PsychotherapyDocument194 pagesJunguian PsychotherapyRene Galvan Heim100% (13)
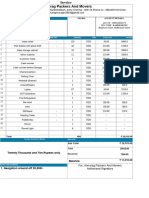
- Flavors Supplies BudgetDocument6 pagesFlavors Supplies BudgetJomarie EmilianoNo ratings yet
- Computer Organization and Assembly Language: Lecture 1 - Basic ConceptsDocument13 pagesComputer Organization and Assembly Language: Lecture 1 - Basic ConceptsNosreffejDelRosarioNo ratings yet
- MKTM028 FathimathDocument23 pagesMKTM028 FathimathShyamly DeepuNo ratings yet
- ANNEX III-Site Components Drawings SetDocument96 pagesANNEX III-Site Components Drawings SetDenice Erika ManzanoNo ratings yet
- Guidelines For Selecting Materials For Downhole Completions Equipment (Jewellery)Document32 pagesGuidelines For Selecting Materials For Downhole Completions Equipment (Jewellery)Slim.BNo ratings yet
- Managerial Economics L4 Consumer BehaviourDocument50 pagesManagerial Economics L4 Consumer BehaviourRifat al haque DhruboNo ratings yet
- Mark Dyczkowski and Trika Journal March 2015 Vol.1.No.1.Document10 pagesMark Dyczkowski and Trika Journal March 2015 Vol.1.No.1.Mark Dyczkoswki and Trika Journal100% (2)
- Direct Marketing: Mcgraw-Hill/IrwinDocument30 pagesDirect Marketing: Mcgraw-Hill/IrwinJunaid KhalidNo ratings yet
- Standard JKR Spec For Bridge LoadingDocument5 pagesStandard JKR Spec For Bridge LoadingHong Rui ChongNo ratings yet
- Kiro Urdin BookDocument189 pagesKiro Urdin BookDane BrdarskiNo ratings yet
- Yingli CS Centrale-Poggiorsini EN 062011-1 PDFDocument2 pagesYingli CS Centrale-Poggiorsini EN 062011-1 PDFZvonko Trajkov100% (1)
- GeM Bidding 3702669Document10 pagesGeM Bidding 3702669ANIMESH JAINNo ratings yet
- Goethe Zertifikat b1 HorenDocument2 pagesGoethe Zertifikat b1 HorenLevent75% (4)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (16)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)