You might also like
- Asia Small and Medium-Sized Enterprise Monitor 2020: Volume II: COVID-19 Impact on Micro, Small, and Medium-Sized Enterprises in Developing AsiaFrom EverandAsia Small and Medium-Sized Enterprise Monitor 2020: Volume II: COVID-19 Impact on Micro, Small, and Medium-Sized Enterprises in Developing AsiaNo ratings yet
- A. Public Service Ministries/AgenciesDocument11 pagesA. Public Service Ministries/AgenciesmonyNo ratings yet
- Provincial Facilitation for Investment and Trade Index: Measuring Economic Governance for Business Development in the Lao People’s Democratic Republic-Second EditionFrom EverandProvincial Facilitation for Investment and Trade Index: Measuring Economic Governance for Business Development in the Lao People’s Democratic Republic-Second EditionNo ratings yet
- A. Public Service Ministries/AgenciesDocument11 pagesA. Public Service Ministries/AgenciesmonyNo ratings yet
- Re-invigorating Private Sector Investment: Private Sector Assessment in FijiFrom EverandRe-invigorating Private Sector Investment: Private Sector Assessment in FijiNo ratings yet
- 2020 1604cfDocument4 pages2020 1604cfRosenda MantosNo ratings yet
- Change / Ammendment Form For Account Office Government of Punjab DoctorsDocument1 pageChange / Ammendment Form For Account Office Government of Punjab DoctorsMuhammad Inaam Ur Rehman80% (5)
- Hide This ColumnDocument412 pagesHide This ColumnKahinu MogesNo ratings yet
- Deputy Director of Textiles (Sericulture), Pay Slip Government of West BengalDocument1 pageDeputy Director of Textiles (Sericulture), Pay Slip Government of West BengalTarun SinhaNo ratings yet
- MfptypfileDocument2 pagesMfptypfileShreyas ChandorkarNo ratings yet
- Candidates Enrolment List for Intake 02/2020Document59 pagesCandidates Enrolment List for Intake 02/2020SOURAVNo ratings yet
- Bir Form 1702-RtDocument8 pagesBir Form 1702-RtJonalyn Lapidario100% (2)
- Ldasr00347890000010105 2018Document1 pageLdasr00347890000010105 2018amar jeetNo ratings yet
- Case study 3 SolutionDocument2 pagesCase study 3 Solutiongaurilakhmani2003No ratings yet
- Statement - Summit School Jahan Khan CampusDocument1 pageStatement - Summit School Jahan Khan CampusSheraz AhmadNo ratings yet
- VANT!: Fe E'D) S In'M It EdDocument21 pagesVANT!: Fe E'D) S In'M It EdJyoti KumariNo ratings yet
- A. Public Service Ministries/AgenciesDocument10 pagesA. Public Service Ministries/AgenciesJeffrey KrauseNo ratings yet
- Jadual Seminar Oktober 2020 - Februari 2021 Institute of Continuing Education & Professional Studies (Iceps) Uitm Shah AlamDocument3 pagesJadual Seminar Oktober 2020 - Februari 2021 Institute of Continuing Education & Professional Studies (Iceps) Uitm Shah Alamnur fatinNo ratings yet
- Public Accounts For B.C.Document17 pagesPublic Accounts For B.C.CTV VancouverNo ratings yet
- Biodata of OfficerDocument2 pagesBiodata of OfficerJoselito de VeraNo ratings yet
- Human Resource Management Section: VoucherDocument8 pagesHuman Resource Management Section: VoucherReia RuecoNo ratings yet
- West Bengal govt pay slip breakdownDocument1 pageWest Bengal govt pay slip breakdownArkit BasuNo ratings yet
- HEALTHCARE SERVICESDocument2 pagesHEALTHCARE SERVICESraviNo ratings yet
- Nov 2019Document1 pageNov 2019Nandan SarkarNo ratings yet
- Indofood Index Profile and Financial HighlightsDocument2 pagesIndofood Index Profile and Financial HighlightsRizki AbirawaNo ratings yet
- January Investment ReportDocument6 pagesJanuary Investment ReportAnonymous dp5b3X1NANo ratings yet
- Government Pay Slip for Amit Kumar NathDocument1 pageGovernment Pay Slip for Amit Kumar NathDebnath DebnathNo ratings yet
- Modified ATCs for CREATE ActDocument2 pagesModified ATCs for CREATE Actjoy rellosoNo ratings yet
- Economic and Financial Data For PolandDocument10 pagesEconomic and Financial Data For Polandh3493061No ratings yet
- Annexure 3 - E-GovernmentDocument1 pageAnnexure 3 - E-GovernmentDocumentsZANo ratings yet
- This Study Resource Was: Josh Murray 7620 Vincent Ave Richfield, MN 55425Document3 pagesThis Study Resource Was: Josh Murray 7620 Vincent Ave Richfield, MN 55425John BeanNo ratings yet
- Wbcal00462120000020786 2018Document1 pageWbcal00462120000020786 2018INDRAJIT NANDANNo ratings yet
- Personal confidential increment letterDocument2 pagesPersonal confidential increment letterAshish SinghNo ratings yet
- Subject: Merit IncreaseDocument2 pagesSubject: Merit IncreaseAshish SinghNo ratings yet
- Contractor'S Plant and Machinery Insurance Policy (Floater Basis)Document2 pagesContractor'S Plant and Machinery Insurance Policy (Floater Basis)Nundeep RakshitNo ratings yet
- March Investment ReportDocument7 pagesMarch Investment ReportAnonymous dp5b3X1NANo ratings yet
- RMC No. 101-2020Document3 pagesRMC No. 101-2020Kenneth FabiaNo ratings yet
- Flash Note - HMB 2QCY22 Result Review - 19-Aug-2022Document3 pagesFlash Note - HMB 2QCY22 Result Review - 19-Aug-2022Mubashir AlamNo ratings yet
- Income Tax Computation FormatDocument2 pagesIncome Tax Computation Formatrathan100% (1)
- Malasakit Program OfficeDocument1 pageMalasakit Program OfficeTor YulsNo ratings yet
- Subject: Merit Increase: Emp Code: 901105 Name: Ashish Kumar Singh Designation: Officer Department: ProductionDocument4 pagesSubject: Merit Increase: Emp Code: 901105 Name: Ashish Kumar Singh Designation: Officer Department: ProductionAshish SinghNo ratings yet
- 02 07 2013 Application LeaveDocument3 pages02 07 2013 Application LeaveSafety Bharatpur OCPNo ratings yet
- Factsheet - 0305709591 - CONG TY CO PHAN PHONG PHU SAC VIET - Company ReportDocument10 pagesFactsheet - 0305709591 - CONG TY CO PHAN PHONG PHU SAC VIET - Company ReportHung NguyenNo ratings yet
- Mercy KaneneDocument1 pageMercy KaneneMercy KaneneNo ratings yet
- Payslip 202003Document3 pagesPayslip 202003muhammad adisukmaNo ratings yet
- PAYSLIPDocument3 pagesPAYSLIPAdi SukmaNo ratings yet
- Salary SlipDocument2 pagesSalary SlipRuchi SinglaNo ratings yet
- Slip Gaji Kapal Api GroupDocument3 pagesSlip Gaji Kapal Api GroupSintyaa100% (1)
- Collateral ManagersDocument3 pagesCollateral ManagersZerohedgeNo ratings yet
- Grand Total 7,364 2,251 0 0 5,087Document1 pageGrand Total 7,364 2,251 0 0 5,087NITIN BOSENo ratings yet
- Salary details and tax computationDocument8 pagesSalary details and tax computationSHELESH GARGNo ratings yet
- THTHA02040910000013386 NewDocument3 pagesTHTHA02040910000013386 NewMR ANIkETNo ratings yet
- THTHA02040910000013386 NewDocument3 pagesTHTHA02040910000013386 NewMR ANIkETNo ratings yet
- PT Kiat Ananda Cold Storage Payroll SlipDocument1 pagePT Kiat Ananda Cold Storage Payroll SlipAde SuharyadiNo ratings yet
- Transaction Statement1626153268Document2 pagesTransaction Statement1626153268Rohit PalNo ratings yet
- Annex-8B-SAN-NICOLAS - Doc Page 4 Lang Po Tita Ang Iprint Po NG 3 Copies Po para Sa Folder NG San Nicolas National High SchoolDocument4 pagesAnnex-8B-SAN-NICOLAS - Doc Page 4 Lang Po Tita Ang Iprint Po NG 3 Copies Po para Sa Folder NG San Nicolas National High SchoolMr. Jaymar AragoNo ratings yet
- Sys PC101 PDFDocument3 pagesSys PC101 PDFRaj EevNo ratings yet
- PSPCL bill detailsDocument2 pagesPSPCL bill detailsGurvinder SinghNo ratings yet
- Receipt No/ Date Seal and Signature of Receiving OfficialDocument10 pagesReceipt No/ Date Seal and Signature of Receiving OfficialRAMAPPA100% (2)
- April Investment ReportDocument7 pagesApril Investment ReportAnonymous dp5b3X1NANo ratings yet
- COA Circular 92-382 Local Government FundsDocument13 pagesCOA Circular 92-382 Local Government FundsDenni Dominic Martinez LeponNo ratings yet
- Strengthening Philippines Secured Transactions LawDocument10 pagesStrengthening Philippines Secured Transactions LawAl MarvinNo ratings yet
- Renew Notary Commission Certificate RequestDocument4 pagesRenew Notary Commission Certificate RequestJhoana Parica Francisco100% (2)
- Etix - Print at Home TicketingDocument2 pagesEtix - Print at Home TicketingAl MarvinNo ratings yet
- Consumer LawsDocument15 pagesConsumer LawsOllie DegsiNo ratings yet
- Bir RR 18 13Document13 pagesBir RR 18 13Chriselle Marie DabaoNo ratings yet
- Re: Registration of Second Amendment To The Real Estate Mortgage of Sps. Lilian B. and Filamer Amado P. BulaoDocument2 pagesRe: Registration of Second Amendment To The Real Estate Mortgage of Sps. Lilian B. and Filamer Amado P. BulaoAl MarvinNo ratings yet
- Affidavit of Joint Undertaking of The PCODocument4 pagesAffidavit of Joint Undertaking of The PCORachelHechanova100% (5)
- Republic of The PhilippinesDocument1 pageRepublic of The PhilippinesKezia Magsayo LumasagNo ratings yet
- NDA-40Document2 pagesNDA-40shinsei123No ratings yet
- NDA-40Document2 pagesNDA-40shinsei123No ratings yet
- Sample Mo A TemplateDocument2 pagesSample Mo A TemplateardiandwikmNo ratings yet
- Acknowledgment Receipt With Release Waiver and Quitclaim: (NAME)Document2 pagesAcknowledgment Receipt With Release Waiver and Quitclaim: (NAME)Al Marvin100% (2)
- 1934415077877096057Document15 pages1934415077877096057Al MarvinNo ratings yet
- Quitclaim (Jobell de Jesus ( (Speedy)Document6 pagesQuitclaim (Jobell de Jesus ( (Speedy)Jennifer TinaganNo ratings yet
- NDA-40Document2 pagesNDA-40shinsei123No ratings yet
- Position Paper On The Transfer of Condominium PropertyDocument2 pagesPosition Paper On The Transfer of Condominium PropertyAl MarvinNo ratings yet
- SwornDocument2 pagesSwornAbegail LeriosNo ratings yet
- W1O C-C-'!"'I'V : QcourtDocument11 pagesW1O C-C-'!"'I'V : QcourtAl MarvinNo ratings yet
- DBP Frontline Services GuideDocument34 pagesDBP Frontline Services GuideDiAne PulidoNo ratings yet
- Heinous Crimes Act - R.A. No. 7659Document15 pagesHeinous Crimes Act - R.A. No. 7659Onireblabas Yor OsicranNo ratings yet
- TableDocument27 pagesTableAl MarvinNo ratings yet
- The Philippine Council For NGO Certification (PCNC) & The Philippine Tax CodeDocument4 pagesThe Philippine Council For NGO Certification (PCNC) & The Philippine Tax CodeKarissa TolentinoNo ratings yet
- Sample Mo A TemplateDocument2 pagesSample Mo A TemplateardiandwikmNo ratings yet
- Republic of The PhilippinesDocument1 pageRepublic of The PhilippinesKezia Magsayo LumasagNo ratings yet
- Demand Letter AgainstDocument1 pageDemand Letter AgainstAl MarvinNo ratings yet
- BSP Circular No. 970-17 Enhanced Corporate GovernanceDocument36 pagesBSP Circular No. 970-17 Enhanced Corporate GovernanceAl MarvinNo ratings yet
- FAQs on Fidelity Bonding for Public OfficialsDocument3 pagesFAQs on Fidelity Bonding for Public OfficialsRapha JohnNo ratings yet
- Their Role in National Development) StatesDocument5 pagesTheir Role in National Development) StatesAl MarvinNo ratings yet
- Goldman-Cecil Medicine 25th 2015Document39 pagesGoldman-Cecil Medicine 25th 2015Dumitru HarsenieNo ratings yet
- Psyc 331 Exam 2 Study GuideDocument2 pagesPsyc 331 Exam 2 Study GuidedivssssssNo ratings yet
- Procedural SedationDocument35 pagesProcedural SedationheshamNo ratings yet
- 11 Antihypertensive AgentsDocument43 pages11 Antihypertensive AgentsnidsNo ratings yet
- Anatomy Pathophysiology PreeclampsiaDocument4 pagesAnatomy Pathophysiology PreeclampsiaKeith Wesley YbutNo ratings yet
- Reflection PaperDocument8 pagesReflection Paperapi-508903095No ratings yet
- 10 - Growth & Reproduction Exercise 4-1Document2 pages10 - Growth & Reproduction Exercise 4-1rhdoiuaNo ratings yet
- Handbook of Patient Care in Cardiac Surgery by John H. Lemmer JR., Gus J. VlahakesDocument379 pagesHandbook of Patient Care in Cardiac Surgery by John H. Lemmer JR., Gus J. Vlahakesyoshizzle129909No ratings yet
- APC Pharmacy Intern Written Exam SampleDocument62 pagesAPC Pharmacy Intern Written Exam SampleDaisy Lu81% (16)
- Government College of Nursing:, Jodhpur (Raj.)Document43 pagesGovernment College of Nursing:, Jodhpur (Raj.)priyankaNo ratings yet
- Dialysis Disequilibrium Syndrome (DDS): Causes, Diagnosis and TreatmentDocument2 pagesDialysis Disequilibrium Syndrome (DDS): Causes, Diagnosis and TreatmentNathaniel SanchezNo ratings yet
- Simulation in Health Care Education: Perspectives in Biology and Medicine February 2008Document6 pagesSimulation in Health Care Education: Perspectives in Biology and Medicine February 2008Birendra MahatNo ratings yet
- Hypertension in Pregnancy: Pathophysiology and Treatment: Stephanie Braunthal and Andrei BrateanuDocument15 pagesHypertension in Pregnancy: Pathophysiology and Treatment: Stephanie Braunthal and Andrei BrateanuAini EvellynNo ratings yet
- J Clinic Periodontology - 2023 - RattuDocument19 pagesJ Clinic Periodontology - 2023 - RattutzulinNo ratings yet
- Kumpulan Jurnal DengueDocument122 pagesKumpulan Jurnal DengueMas MantriNo ratings yet
- Forensic PsychiatryDocument5 pagesForensic PsychiatrySheba Dan de WiseNo ratings yet
- Cosmetic Surgery An Interdisciplinary ApproachDocument1,004 pagesCosmetic Surgery An Interdisciplinary ApproachDaniel FilizzolaNo ratings yet
- 2021 - СРРРРРРС - 3 Course - GM - EnglDocument17 pages2021 - СРРРРРРС - 3 Course - GM - EnglAiganym AmanovaNo ratings yet
- DyspneuDocument9 pagesDyspneuAmy KochNo ratings yet
- Demonstration On Chest Physiotherapy DefinitionDocument3 pagesDemonstration On Chest Physiotherapy Definitiondileep0% (1)
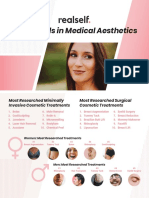
- RealSelf YearInReview OneSheetDocument2 pagesRealSelf YearInReview OneSheetDominico Adityo RaharjoNo ratings yet
- Risk Assessment Matrix (ISO) - 3Document1 pageRisk Assessment Matrix (ISO) - 3Verina GaldasNo ratings yet
- ORTHODONTICS CLASSIFICATION REVISITEDDocument7 pagesORTHODONTICS CLASSIFICATION REVISITEDDharampal SinghNo ratings yet
- Neurogenic BladderDocument15 pagesNeurogenic BladderPutri Wulandari100% (1)
- Leopold's Maneuver ResearchDocument4 pagesLeopold's Maneuver ResearchCarl Andre ReyesNo ratings yet
- BSC Perfusion TechnologyDocument78 pagesBSC Perfusion TechnologyTanisha ShaikhNo ratings yet
- 5 1 1113Document7 pages5 1 1113Adhitya Rizky IsnandyaNo ratings yet
- Fetal DistressDocument32 pagesFetal DistressMadhu Sudhan PandeyaNo ratings yet
- Cna Practice ExamDocument4 pagesCna Practice ExamJennifer Venfield83% (12)
- Cram Reviewer MusculoskeletalDocument32 pagesCram Reviewer MusculoskeletalGwynthselle SalazarNo ratings yet