You might also like
- Disease Detectives NotesDocument5 pagesDisease Detectives NotesErica Weng0% (1)
- Mixing Tank 2 Mixing Tank 1: Chemical ChemicalDocument1 pageMixing Tank 2 Mixing Tank 1: Chemical ChemicalFahrunnisa AdzqiaNo ratings yet
- Serrum Ferritin: A Prognostic Marker in Patients With Sepsis in Pediatric Age Group: A Prospective Cohort StudyDocument4 pagesSerrum Ferritin: A Prognostic Marker in Patients With Sepsis in Pediatric Age Group: A Prospective Cohort StudyclaudyNo ratings yet
- Mortalidad PardsDocument9 pagesMortalidad PardsBarbara Seminario RamirezNo ratings yet
- Application of Different Scoring Systems and Their Value in Pediatric Intensive Care UnitDocument6 pagesApplication of Different Scoring Systems and Their Value in Pediatric Intensive Care UnitPreksha AdeNo ratings yet
- Escala BronquiolitisDocument13 pagesEscala BronquiolitisconfesionesdeunatreintaneraNo ratings yet
- Sankar 2019Document8 pagesSankar 2019Janny Torres AvilaNo ratings yet
- Severe Sepsis-Associated Morbidity and Mortality Among Critically Ill Children With CancerDocument8 pagesSevere Sepsis-Associated Morbidity and Mortality Among Critically Ill Children With CancerFaki D'pasnizerNo ratings yet
- Clinical Characteristics of Covid 19 Infection in The Pediatric Age Group 11019Document4 pagesClinical Characteristics of Covid 19 Infection in The Pediatric Age Group 11019Alina BabilevNo ratings yet
- Severity of Illness and Organ Dysfunction Scoring in ChildrenDocument9 pagesSeverity of Illness and Organ Dysfunction Scoring in Childrenmr_curiousityNo ratings yet
- A Novel Severity Score To Predict Inpatient Mortality in COVID 19 PatientsDocument8 pagesA Novel Severity Score To Predict Inpatient Mortality in COVID 19 PatientsanscstNo ratings yet
- Aborto septico Lanari-USA ICM 2004Document6 pagesAborto septico Lanari-USA ICM 2004pastorizaariana25No ratings yet
- Bacterial Etiology of Pediatric Subacute Hematogenous OsteomyelitisDocument6 pagesBacterial Etiology of Pediatric Subacute Hematogenous OsteomyelitismiNo ratings yet
- BMJ m3249 FullDocument15 pagesBMJ m3249 Fullvuongquynh290900No ratings yet
- Prognostic of Sepsis in A Congolese Pediatric Emergency Service Using PSOFA Score A Prospective StudyDocument6 pagesPrognostic of Sepsis in A Congolese Pediatric Emergency Service Using PSOFA Score A Prospective StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Yogaraj 2002Document7 pagesYogaraj 2002زينب محمد عبدNo ratings yet
- Risk Factors For Necrotizing Enterocolitis Associated MortalityDocument7 pagesRisk Factors For Necrotizing Enterocolitis Associated MortalityvaleriaNo ratings yet
- 140970.2 20201002121019 Covered PDFDocument10 pages140970.2 20201002121019 Covered PDFLee제노No ratings yet
- Fmab 066Document9 pagesFmab 066vuongquynh290900No ratings yet
- q1. Intensive CareDocument10 pagesq1. Intensive CareMari Carmen GrandasNo ratings yet
- GuiasddddDocument10 pagesGuiasddddKarla CastilloNo ratings yet
- Incidence, Outcome and Risk Factors For Sepsis - A Two Year Retrospective Study at Surgical ICU of A Tertiary Hospital in Pakistan.Document6 pagesIncidence, Outcome and Risk Factors For Sepsis - A Two Year Retrospective Study at Surgical ICU of A Tertiary Hospital in Pakistan.faraz.mirza1No ratings yet
- PIRO Classification Predicts Outcomes in Pediatric SepsisDocument7 pagesPIRO Classification Predicts Outcomes in Pediatric SepsisDiana Paola Castaño SalazarNo ratings yet
- National Survey of Factors Associated With Repeated Admissions Due To Febrile SeizureDocument4 pagesNational Survey of Factors Associated With Repeated Admissions Due To Febrile Seizurehilman lesmanaNo ratings yet
- Quantitative Sars-Cov-2 Serology in Children With Multisystem in Ammatory Syndrome (Mis-C)Document11 pagesQuantitative Sars-Cov-2 Serology in Children With Multisystem in Ammatory Syndrome (Mis-C)FC Mekar AbadiNo ratings yet
- Neonatal Sepsis Prevalence in EthiopiaDocument11 pagesNeonatal Sepsis Prevalence in EthiopiarullyNo ratings yet
- 1 s2.0 S0021755722000031 MainDocument9 pages1 s2.0 S0021755722000031 MainMaría Pía BalmacedaNo ratings yet
- 3 Septicshock SIRS PDFDocument11 pages3 Septicshock SIRS PDFRhobbigfirly UnggulNo ratings yet
- COVID-19-Associated Multisystem Inflammatory Syndrome in Children - United States, March-July 2020Document7 pagesCOVID-19-Associated Multisystem Inflammatory Syndrome in Children - United States, March-July 2020Alejandro LondoñoNo ratings yet
- Candidiasis in PICUDocument6 pagesCandidiasis in PICUMeirinda HidayantiNo ratings yet
- PIIS0022347620315432Document8 pagesPIIS0022347620315432Suwandi ChangNo ratings yet
- 204 FullDocument10 pages204 FullJose Carlos Soto SaenzNo ratings yet
- 5754-Article Text-43741-3-10-20220520Document18 pages5754-Article Text-43741-3-10-20220520Ricardo TanNo ratings yet
- BJC 2017154Document8 pagesBJC 2017154Altair CamargoNo ratings yet
- Fmab 025Document9 pagesFmab 025gabopeluditoNo ratings yet
- Acta Paediatr 2006 p208Document6 pagesActa Paediatr 2006 p208Handris SupriadiNo ratings yet
- Chronic Kidney Disease Is Associated With A Higher 90-Day Mortality Than Other Chronic Medical Conditions in Patients With SepsisDocument8 pagesChronic Kidney Disease Is Associated With A Higher 90-Day Mortality Than Other Chronic Medical Conditions in Patients With Sepsisida ayu agung WijayantiNo ratings yet
- Fitzgerald 2019Document10 pagesFitzgerald 2019senkonenNo ratings yet
- Research Article: The Analysis of Etiology and Risk Factors For 192 Cases of Neonatal SepsisDocument7 pagesResearch Article: The Analysis of Etiology and Risk Factors For 192 Cases of Neonatal Sepsisflorentina lulutNo ratings yet
- Oup Accepted Manuscript 2018Document12 pagesOup Accepted Manuscript 2018DaVid Mo-RaNo ratings yet
- Pinda FynDocument7 pagesPinda FynCaballero X CaballeroNo ratings yet
- 10 11648 J Ijidt 20200501 12Document5 pages10 11648 J Ijidt 20200501 12hern andesNo ratings yet
- Prevalencia de Sepsis Grave en Las Unidades de Cuidado Intensivo. Primer Estudio Nacional MulticéntricoDocument11 pagesPrevalencia de Sepsis Grave en Las Unidades de Cuidado Intensivo. Primer Estudio Nacional MulticéntricoMayra CondeNo ratings yet
- 2021 Article 2702Document7 pages2021 Article 2702Gangga ChandraNo ratings yet
- Bacterial Complications of Primary Varicella in ChildrenDocument8 pagesBacterial Complications of Primary Varicella in ChildrenntnquynhproNo ratings yet
- During The Coronavirus Disease 2019 (COVID-19) Pandemic, A New Phenomenon Manifesting As ADocument5 pagesDuring The Coronavirus Disease 2019 (COVID-19) Pandemic, A New Phenomenon Manifesting As APratiwiNo ratings yet
- 00002Document5 pages00002Oscar F. Vargas AlvaradoNo ratings yet
- Brief ReportsDocument19 pagesBrief Reportsdery sernaNo ratings yet
- Jurnal Pediatric BaruDocument8 pagesJurnal Pediatric BaruHhhNo ratings yet
- Severe and Fatal Forms of Covid-19 in Children: SciencedirectDocument4 pagesSevere and Fatal Forms of Covid-19 in Children: Sciencedirectrianza hutasuhutNo ratings yet
- Hospital Admission in Children and Adolescents With COVID-19Document2 pagesHospital Admission in Children and Adolescents With COVID-19Diana OlivaresNo ratings yet
- MM 2Document5 pagesMM 2worksheetbookNo ratings yet
- Multisystem Inflammatory Syndrome in U.S. Children and AdolescentsDocument13 pagesMultisystem Inflammatory Syndrome in U.S. Children and AdolescentsHarold CookNo ratings yet
- Achieving Sustainability in Reducing Unplanned Extubations in PICUDocument7 pagesAchieving Sustainability in Reducing Unplanned Extubations in PICUKevin Bazán TorrealvaNo ratings yet
- (10920684 - Neurosurgical Focus) Predictors of Outcome of Subdural Empyema in ChildrenDocument6 pages(10920684 - Neurosurgical Focus) Predictors of Outcome of Subdural Empyema in ChildrenFatima RamirezNo ratings yet
- Ioi80197 463 473Document11 pagesIoi80197 463 473Phạm LinhNo ratings yet
- 385 - Epidemiology of Burn-Injured Children in U.S. PicusDocument1 page385 - Epidemiology of Burn-Injured Children in U.S. PicusE.sundara BharathiNo ratings yet
- Pediatric Sepsis Definition-A Systematic Review Protocol by The Pediatric Sepsis Definition TaskforceDocument7 pagesPediatric Sepsis Definition-A Systematic Review Protocol by The Pediatric Sepsis Definition TaskforceGunduz AgaNo ratings yet
- RequestedDocument9 pagesRequestedGaurav MauryaNo ratings yet
- TITLE: Real-World Effectiveness of Hydroxychloroquine, Azithromycin, and Ivermectin AmongDocument25 pagesTITLE: Real-World Effectiveness of Hydroxychloroquine, Azithromycin, and Ivermectin AmongMigjofNo ratings yet
- Incidence and Risk Factors For Ventilator Associated Pneumon 2007 RespiratorDocument6 pagesIncidence and Risk Factors For Ventilator Associated Pneumon 2007 RespiratorTomasNo ratings yet
- COVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19From EverandCOVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19No ratings yet
- Housfather 2007Document9 pagesHousfather 2007mr_curiousityNo ratings yet
- Self Assesment PDFDocument1 pageSelf Assesment PDFmr_curiousityNo ratings yet
- Skema Hibah PNBP - 2020Document26 pagesSkema Hibah PNBP - 2020mr_curiousityNo ratings yet
- OtologiDocument13 pagesOtologimr_curiousityNo ratings yet
- Bloos 2016Document11 pagesBloos 2016mr_curiousityNo ratings yet
- Hochreiter2009 PDFDocument7 pagesHochreiter2009 PDFmr_curiousityNo ratings yet
- Antibiotics 02 00001Document10 pagesAntibiotics 02 00001Jenny AlmagroNo ratings yet
- Use of Procalcitonin To Shorten Antibiotic Treatment Duration in Septic PatientsDocument8 pagesUse of Procalcitonin To Shorten Antibiotic Treatment Duration in Septic Patientsmr_curiousityNo ratings yet
- Jurnal Bang Yudi 2 PDFDocument5 pagesJurnal Bang Yudi 2 PDFMuhammad Alief FahrenNo ratings yet
- Summ Ah 2009Document10 pagesSumm Ah 2009mr_curiousityNo ratings yet
- Pediatric Sepsis and Multiple Organ Dysfunction SyndromeDocument7 pagesPediatric Sepsis and Multiple Organ Dysfunction Syndromemr_curiousityNo ratings yet
- Severity of Illness and Organ Dysfunction Scoring in ChildrenDocument9 pagesSeverity of Illness and Organ Dysfunction Scoring in Childrenmr_curiousityNo ratings yet
- Serum Procalcitonin in Pneumococcal Pneumonia in Children: M. Korppi, S. RemesDocument5 pagesSerum Procalcitonin in Pneumococcal Pneumonia in Children: M. Korppi, S. Remesmr_curiousityNo ratings yet
- ELS PricelistDocument10 pagesELS PricelistMulyani Dwi SetianingrumNo ratings yet
- Circulating Procalcitonin and Cleavage Products in Septicaemia Compared With Medullary Thyroid CarcinomaDocument5 pagesCirculating Procalcitonin and Cleavage Products in Septicaemia Compared With Medullary Thyroid Carcinomamr_curiousityNo ratings yet
- Serum Procalcitonin in Pneumococcal Pneumonia in Children: M. Korppi, S. RemesDocument5 pagesSerum Procalcitonin in Pneumococcal Pneumonia in Children: M. Korppi, S. Remesmr_curiousityNo ratings yet
- Clinical Value of Procalcitonin For Patients With Suspected Bloodstream InfectionDocument9 pagesClinical Value of Procalcitonin For Patients With Suspected Bloodstream Infectionmr_curiousityNo ratings yet
- Simon 2004Document12 pagesSimon 2004mr_curiousityNo ratings yet
- Diagnostic and Prognostic Biomarkers of Sepsis in Critical CareDocument8 pagesDiagnostic and Prognostic Biomarkers of Sepsis in Critical Caremr_curiousityNo ratings yet
- Procalcitonin Increase After Endotoxin Injection in Normal SubjectsDocument4 pagesProcalcitonin Increase After Endotoxin Injection in Normal Subjectsmr_curiousityNo ratings yet
- Book Reviews: David J. Dries, Book Review EditorDocument2 pagesBook Reviews: David J. Dries, Book Review Editormr_curiousityNo ratings yet
- Nelson Last Minute Pediatrics Guide Covers Key Developmental MilestonesDocument392 pagesNelson Last Minute Pediatrics Guide Covers Key Developmental Milestonesjeyaprakash jayaramanNo ratings yet
- Immunization Programme in NepalDocument13 pagesImmunization Programme in Nepalrina dutta100% (1)
- The Chain of InfectionDocument12 pagesThe Chain of InfectionJacob DichosaNo ratings yet
- Method Statement TemplateDocument3 pagesMethod Statement TemplateKayNo ratings yet
- Lect 8 Pneumonia PDFDocument68 pagesLect 8 Pneumonia PDFRaghad AbdullaNo ratings yet
- Indonesian Pediatric Nutrition and Metabolic Update ConferenceDocument2 pagesIndonesian Pediatric Nutrition and Metabolic Update ConferenceJayantiNo ratings yet
- Site Visit ReportDocument8 pagesSite Visit ReportVijay BanikNo ratings yet
- Effects of Hostel Water on Student Health and FinancesDocument4 pagesEffects of Hostel Water on Student Health and FinancesCephas StoneNo ratings yet
- Pregnancy Guide for Expecting MothersDocument19 pagesPregnancy Guide for Expecting MothersSalma TariqNo ratings yet
- Baby Best ChanceDocument154 pagesBaby Best Chanceband12No ratings yet
- Activity 4.health Education PlanDocument3 pagesActivity 4.health Education Planjoannamae molaga0% (1)
- Practice Exercises For EpidemiologyDocument8 pagesPractice Exercises For Epidemiologyninja-2001100% (2)
- In The Supreme Court of Bermuda: Civil Jurisdiction 2021: No. 162Document38 pagesIn The Supreme Court of Bermuda: Civil Jurisdiction 2021: No. 162BernewsAdminNo ratings yet
- Nursing Care Reduces Labor Pain and CostsDocument14 pagesNursing Care Reduces Labor Pain and Costssgd bsepuluhNo ratings yet
- Area Risk Identification and Mitigation StrategiesDocument12 pagesArea Risk Identification and Mitigation StrategiesBagus Kusuma WardhanaNo ratings yet
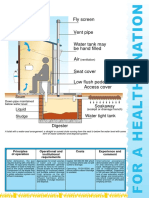
- SA AquaPrivyDocument1 pageSA AquaPrivygkumar77100% (2)
- Pasadena 8 15 12Document2 pagesPasadena 8 15 12Debbie SimmonsNo ratings yet
- Preventing Suicide - A Global Imperative WHO 2014 - 9789241564878 - EngDocument141 pagesPreventing Suicide - A Global Imperative WHO 2014 - 9789241564878 - EngDisability Rights AllianceNo ratings yet
- Nursing Problems of a Family PrioritizedDocument4 pagesNursing Problems of a Family PrioritizedElly Lazaro100% (1)
- Vacuna Moderna Updated CDC September 11, 2023 Clinical Review - SPIKEVAXDocument156 pagesVacuna Moderna Updated CDC September 11, 2023 Clinical Review - SPIKEVAX9jz5dzj5gwNo ratings yet
- 2011 - Unsafe Abortion and Postabortion Care - An OverviewDocument9 pages2011 - Unsafe Abortion and Postabortion Care - An OverviewJeremiah WestNo ratings yet
- PostnatalDocument36 pagesPostnatalAditya BarmanNo ratings yet
- HepBPerinatal ProtectWhenPregnant BWDocument2 pagesHepBPerinatal ProtectWhenPregnant BWKhalidatunnur Andrianie NasihinNo ratings yet
- 02.15 - Labor & DeliveryDocument6 pages02.15 - Labor & DeliveryHoney Semafranca PlatolonNo ratings yet
- NCCN Guidelines On Breast Cancer Risk ReductionDocument64 pagesNCCN Guidelines On Breast Cancer Risk ReductionMary Camille AzarconNo ratings yet
- Factors Associated With Timely Immunization of HIVExposed Infants Attending HIVAIDS Clinic at Ishaka Adventist HospitalDocument11 pagesFactors Associated With Timely Immunization of HIVExposed Infants Attending HIVAIDS Clinic at Ishaka Adventist HospitalKIU PUBLICATION AND EXTENSIONNo ratings yet
- M104 - ExamDocument8 pagesM104 - ExamChrystal Anne Flores CorderoNo ratings yet
- Analysis of HACCP Application in Oriflakes ProductionDocument13 pagesAnalysis of HACCP Application in Oriflakes ProductionindragazaliNo ratings yet
- Learning About HIV: A Lesson Plan From Rights, Respect, Responsibility: A K-12 CurriculumDocument7 pagesLearning About HIV: A Lesson Plan From Rights, Respect, Responsibility: A K-12 CurriculumRazell Jean ArazaNo ratings yet