You might also like
- Breathing RetrainingDocument39 pagesBreathing RetrainingAishwarya PanchalNo ratings yet
- Breathing ExerciseDocument29 pagesBreathing ExerciseJawad MohammadNo ratings yet
- Diaphragm Paralysis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDiaphragm Paralysis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Pulmo Rehab GuideDocument65 pagesPulmo Rehab GuideFarrukh ShahzadNo ratings yet
- Exploring Cupping Today: A Beginners Course On Cupping Therapy & It's BenefitsFrom EverandExploring Cupping Today: A Beginners Course On Cupping Therapy & It's BenefitsNo ratings yet
- Active Cycle of Breathing TechniqueDocument3 pagesActive Cycle of Breathing TechniqueSurya KalaNo ratings yet
- Traditional Chinese Medicine: A Natural Guide to Weight Loss That LastsFrom EverandTraditional Chinese Medicine: A Natural Guide to Weight Loss That LastsNo ratings yet
- Active Movements Active Movements: By: DR - Chaman LalDocument51 pagesActive Movements Active Movements: By: DR - Chaman LalAmbreena RasoolNo ratings yet
- Classical and Modern Theories of AcupunctureDocument11 pagesClassical and Modern Theories of AcupunctureAbhishek Dubey100% (1)
- Ataxia Gait Disturbances: Presented By:-Pradip ChoudharyDocument15 pagesAtaxia Gait Disturbances: Presented By:-Pradip ChoudharynrusinghNo ratings yet
- A Practical Guide to the Self-Management of Lower Back Pain: A Holistic Approach to Health and FitnessFrom EverandA Practical Guide to the Self-Management of Lower Back Pain: A Holistic Approach to Health and FitnessNo ratings yet
- Breathing and Relaxation: Technique 1Document2 pagesBreathing and Relaxation: Technique 1Venkata Nagaraj MummadisettyNo ratings yet
- Active Cycle Breathing TechniqueDocument20 pagesActive Cycle Breathing TechniqueRAM100% (2)
- GaitDocument42 pagesGaitTan Geok EngNo ratings yet
- The Acupuncture Prescription:: A Holistic Approach to HealthFrom EverandThe Acupuncture Prescription:: A Holistic Approach to HealthNo ratings yet
- PELVIC TILTING: ANATOMY, TYPES AND IMPORTANCEDocument28 pagesPELVIC TILTING: ANATOMY, TYPES AND IMPORTANCEvenkata ramakrishnaiahNo ratings yet
- Kinesio Taping (KT)Document32 pagesKinesio Taping (KT)book100% (1)
- Gait AbnormalityDocument5 pagesGait AbnormalityKinshuk BansalNo ratings yet
- The Acupressure Handbook: Ancient Healing Techniques for Today's WorldFrom EverandThe Acupressure Handbook: Ancient Healing Techniques for Today's WorldNo ratings yet
- Pressure On Vital PointsDocument7 pagesPressure On Vital PointskyleNo ratings yet
- Biomech of Hip Pelvic Motions MSDocument18 pagesBiomech of Hip Pelvic Motions MSSyed Alamdar HussainNo ratings yet
- Training Course Mumbai June 2013 & Correspondence CoursesDocument9 pagesTraining Course Mumbai June 2013 & Correspondence CoursesJenneey D RajaniNo ratings yet
- ClaudicationDocument6 pagesClaudicationdvenumohanNo ratings yet
- Flutter and Other DeviceDocument39 pagesFlutter and Other DeviceEira LopezNo ratings yet
- Lecture Notes On NORMAL GAIT by DR M N SiddiquiDocument7 pagesLecture Notes On NORMAL GAIT by DR M N SiddiquiChandni P100% (1)
- Massage and Remedial Exercises: In Medical and Surgical ConditionsFrom EverandMassage and Remedial Exercises: In Medical and Surgical ConditionsRating: 5 out of 5 stars5/5 (2)
- Application Technique Traction PDFDocument25 pagesApplication Technique Traction PDFAZOZ 19No ratings yet
- Shiatsu and Acupressure Two Different and DistinctDocument8 pagesShiatsu and Acupressure Two Different and DistinctEmre YalçınNo ratings yet
- The Leg Three Miles Acupuncture PointDocument5 pagesThe Leg Three Miles Acupuncture Pointcristina_tigruNo ratings yet
- CHINESE Herbal Medicine For Beginners: UNDERSTANDING THE PRINCIPLES AND PRACTICES OF CHINESE HERBAL MEDICINEFrom EverandCHINESE Herbal Medicine For Beginners: UNDERSTANDING THE PRINCIPLES AND PRACTICES OF CHINESE HERBAL MEDICINENo ratings yet
- Diaphragmatic Breathing - The Foundation of Core Stability PDFDocument7 pagesDiaphragmatic Breathing - The Foundation of Core Stability PDFElaine CspNo ratings yet
- APC Cardio Catalina-1Document21 pagesAPC Cardio Catalina-1Carmelo ScavoneNo ratings yet
- A Comprehensive Study On Marma PointsDocument9 pagesA Comprehensive Study On Marma Pointsaaronjdriver2248100% (1)
- 1.laser TherapyDocument12 pages1.laser TherapyFaisal Mehboob67% (3)
- Therapeutic Exercise: The HipDocument39 pagesTherapeutic Exercise: The HipMuhammad UsmanNo ratings yet
- The Art of MassageDocument205 pagesThe Art of MassageYina YounNo ratings yet
- Mike Shoulder Anatomy and Clinical Assessment of The Shoulder Mike BMUS SiG 2017Document46 pagesMike Shoulder Anatomy and Clinical Assessment of The Shoulder Mike BMUS SiG 2017loka jananiNo ratings yet
- Shoulder Dislocation - Mindy LutzDocument17 pagesShoulder Dislocation - Mindy LutzpritammotghareNo ratings yet
- Kinesio TapingDocument26 pagesKinesio Tapingapi-495322975No ratings yet
- Body Posture QuestionnaireDocument4 pagesBody Posture QuestionnaireKhairul Faiz50% (2)
- Acupressure and Reflex Points For Common AilmentsDocument15 pagesAcupressure and Reflex Points For Common AilmentsAnonymous j3gtTwNo ratings yet
- Click Here For A Video Demonstration: UnresponsivenessDocument3 pagesClick Here For A Video Demonstration: UnresponsivenessJnana YumnaNo ratings yet
- TCM Diagnosis PrinciplesDocument59 pagesTCM Diagnosis PrinciplesMarselina Anastasia AndriesNo ratings yet
- Hypertension FinalDocument2 pagesHypertension Finalapi-203207342100% (1)
- Joint Mobilization To The Elbow, Wrist and Hand2Document43 pagesJoint Mobilization To The Elbow, Wrist and Hand2Tripty Khanna Karwal100% (1)
- Tennis Elbow PDFDocument2 pagesTennis Elbow PDFSabau PetreNo ratings yet
- Diagnostic Touch Its Principles and Application PDFDocument9 pagesDiagnostic Touch Its Principles and Application PDFJakobStierleNo ratings yet
- Stroke RehabDocument51 pagesStroke RehabchillycrabNo ratings yet
- Daftar Pustaka: Stroke:background, Epidemiology, Etiology and Avoiding RecurrenceDocument5 pagesDaftar Pustaka: Stroke:background, Epidemiology, Etiology and Avoiding RecurrenceRenaldiPrimaSaputraNo ratings yet
- Physiotherapy Management of SciaticaDocument6 pagesPhysiotherapy Management of SciaticaMuly Arafah ZakariaNo ratings yet
- Cemented Vs CementlessDocument23 pagesCemented Vs CementlessRenaldiPrimaSaputraNo ratings yet
- Boxing Injuries Anatomical Location ReviewDocument8 pagesBoxing Injuries Anatomical Location ReviewRenaldiPrimaSaputraNo ratings yet
- Human Autoimmune Diseases: A Comprehensive Update: ReviewDocument27 pagesHuman Autoimmune Diseases: A Comprehensive Update: Reviewkaren rinconNo ratings yet
- Pain Referral From The Sternoclavicular Joint: A Study in Normal VolunteersDocument4 pagesPain Referral From The Sternoclavicular Joint: A Study in Normal VolunteersRenaldiPrimaSaputraNo ratings yet
- Physiotherapy Management of SciaticaDocument6 pagesPhysiotherapy Management of SciaticaMuly Arafah ZakariaNo ratings yet
- Influence of Seasonal Changes On Disease Activity and Distribution of Affected Joints in Rheumatoid ArthritisDocument8 pagesInfluence of Seasonal Changes On Disease Activity and Distribution of Affected Joints in Rheumatoid ArthritisRenaldiPrimaSaputraNo ratings yet
- A Proposed Classifi Cation of The Immunological Diseases: Research in TranslationDocument7 pagesA Proposed Classifi Cation of The Immunological Diseases: Research in TranslationRenaldiPrimaSaputraNo ratings yet
- Human Autoimmune Diseases: A Comprehensive Update: ReviewDocument27 pagesHuman Autoimmune Diseases: A Comprehensive Update: Reviewkaren rinconNo ratings yet
- Mechanical Tension and Spontaneous Muscle Twitching Precede The Formation of Cross-Striated Muscle in VivoDocument53 pagesMechanical Tension and Spontaneous Muscle Twitching Precede The Formation of Cross-Striated Muscle in VivoRenaldiPrimaSaputraNo ratings yet
- Physiotherapy Management For COVID-19 in The Acute Hospital Setting: Clinical Practice RecommendationsDocument10 pagesPhysiotherapy Management For COVID-19 in The Acute Hospital Setting: Clinical Practice RecommendationsRenaldiPrimaSaputraNo ratings yet
- Work-Related Musculoskeletal Disorders Among Tea PluckersDocument12 pagesWork-Related Musculoskeletal Disorders Among Tea PluckersRenaldiPrimaSaputraNo ratings yet
- Autoimmune and Rheumatic Musculoskeletal Diseases As A Consequence of SARS-CoV-2 Infection and Its TreatmentDocument16 pagesAutoimmune and Rheumatic Musculoskeletal Diseases As A Consequence of SARS-CoV-2 Infection and Its TreatmentSAMUEL ESCARESNo ratings yet
- Ergonomics, Biomechanics & Musculoskeletal Disorder-A ReviewDocument8 pagesErgonomics, Biomechanics & Musculoskeletal Disorder-A ReviewRenaldiPrimaSaputraNo ratings yet
- Design and Evaluation of Ergonomic Interventions For The Prevention of Musculoskeletal Disorders in IndiaDocument7 pagesDesign and Evaluation of Ergonomic Interventions For The Prevention of Musculoskeletal Disorders in IndiaRenaldiPrimaSaputraNo ratings yet
- UNDERLYINGDocument1 pageUNDERLYINGRenaldiPrimaSaputraNo ratings yet
- E039 PublishedDocument8 pagesE039 PublishedRenaldiPrimaSaputraNo ratings yet
- Afzal Et Al Int. J. Med. Appl. Health. Vol. 4, No. 2, 2016Document2 pagesAfzal Et Al Int. J. Med. Appl. Health. Vol. 4, No. 2, 2016RenaldiPrimaSaputraNo ratings yet
- Cervical Radiculopathy: Cervical Injuries and Treatment (HJ Kim, Section Editor)Document9 pagesCervical Radiculopathy: Cervical Injuries and Treatment (HJ Kim, Section Editor)bandiiitzNo ratings yet
- Tool Design For Tea Cutting Machine To Reduce Msds Using Ergonomic Function Deployment: A Research at PTPN 8 CiaterDocument4 pagesTool Design For Tea Cutting Machine To Reduce Msds Using Ergonomic Function Deployment: A Research at PTPN 8 CiaterRenaldiPrimaSaputraNo ratings yet
- Vertigo: A Review of Common Peripheral and Central Vestibular DisordersDocument7 pagesVertigo: A Review of Common Peripheral and Central Vestibular DisordersPutra ImanullahNo ratings yet
- Chen 2013Document5 pagesChen 2013RenaldiPrimaSaputraNo ratings yet
- Tiyas Masaid UNDERLYINGDocument1 pageTiyas Masaid UNDERLYINGRenaldiPrimaSaputraNo ratings yet
- Meniscus InjuriesDocument10 pagesMeniscus InjuriesRenaldiPrimaSaputraNo ratings yet
- The Somatic Connection: Manual Therapy Is Beneficial For Cervical RadiculopathyDocument3 pagesThe Somatic Connection: Manual Therapy Is Beneficial For Cervical RadiculopathyRenaldiPrimaSaputraNo ratings yet
- Review of Cervical Radiculopathy Causes, Diagnosis and TreatmentDocument8 pagesReview of Cervical Radiculopathy Causes, Diagnosis and TreatmentRenaldiPrimaSaputraNo ratings yet
- Safety Measure Questionnaire 2016Document2 pagesSafety Measure Questionnaire 2016murali100% (3)
- Uts Pen Ilmiah Rinaldi 2109047029Document2 pagesUts Pen Ilmiah Rinaldi 2109047029RenaldiPrimaSaputraNo ratings yet
- Blood Flow Restriction TherapyDocument5 pagesBlood Flow Restriction TherapyRenaldiPrimaSaputraNo ratings yet
- Detector Balance Induccion.Document11 pagesDetector Balance Induccion.Jesus OrtizNo ratings yet
- PEC ReviewerDocument17 pagesPEC ReviewerJunallyn ManigbasNo ratings yet
- ISC 2023 English Language Question PaperDocument5 pagesISC 2023 English Language Question PaperMohit JoshiNo ratings yet
- Next Best Action in An Omnichannel EnvironmentDocument40 pagesNext Best Action in An Omnichannel EnvironmentMadhu100% (2)
- Statement of Financial Affairs: United States Bankruptcy Court Southern District of New YorkDocument42 pagesStatement of Financial Affairs: United States Bankruptcy Court Southern District of New YorkChapter 11 DocketsNo ratings yet
- Surface Modification of Titanium Orthodontic ImplaDocument30 pagesSurface Modification of Titanium Orthodontic ImplaMary SmileNo ratings yet
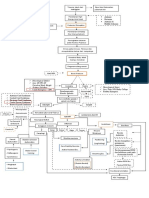
- Generator System Fault Calculation Design GuideDocument22 pagesGenerator System Fault Calculation Design Guidedheerajdorlikar100% (2)
- The Columbian Exchange ReadingDocument3 pagesThe Columbian Exchange Readingapi-286657372No ratings yet
- Phil. Crocodile-WPS OfficeDocument19 pagesPhil. Crocodile-WPS OfficeQUEENIE JAM ABENOJANo ratings yet
- Eastern Shipping Lines, Inc. v. IAC, G.R. No. L-69044 and L-71478, May 29, 1987, 150 SCRA 463Document11 pagesEastern Shipping Lines, Inc. v. IAC, G.R. No. L-69044 and L-71478, May 29, 1987, 150 SCRA 463Melle EscaroNo ratings yet
- Fire and Ice by Robert FrostDocument2 pagesFire and Ice by Robert Frostapi-561976496No ratings yet
- ZEOLITEDocument13 pagesZEOLITEShubham Yele100% (1)
- Weak Downlink Data for Multiple TRX Indices Over TimeDocument3,643 pagesWeak Downlink Data for Multiple TRX Indices Over TimeSK Basak BDNo ratings yet
- Paper 1R MSDocument25 pagesPaper 1R MSAkashNo ratings yet
- Clarke 1973 Loss of InnocenceDocument13 pagesClarke 1973 Loss of InnocencePaula TralmaNo ratings yet
- Ideas For Income Generating Projects PDFDocument29 pagesIdeas For Income Generating Projects PDFheart AquinoNo ratings yet
- Input Interfaces - Locate LPN LockDocument22 pagesInput Interfaces - Locate LPN LockSatyanarayana NekkantiNo ratings yet
- Kole 2010Document12 pagesKole 2010Steven Mestres-JunqueNo ratings yet
- Cost Concepts, Cost Analysis, and Cost EstimationDocument2 pagesCost Concepts, Cost Analysis, and Cost EstimationGêmTürÏngånÖNo ratings yet
- Warsaw Pact Order of Battle - 1989Document61 pagesWarsaw Pact Order of Battle - 1989Zero Knight100% (1)
- Industrial Radiography Image Forming Techniques English 4Document114 pagesIndustrial Radiography Image Forming Techniques English 4Narasimha Murthy InampudiNo ratings yet
- Complicaciones en La Tracción Ortodóntica Del Canino Superior Izquierdo. Retratamiento.Document7 pagesComplicaciones en La Tracción Ortodóntica Del Canino Superior Izquierdo. Retratamiento.Miltonfcc100% (1)
- Syllabus For ETABSDocument2 pagesSyllabus For ETABSSandgrouse RajNo ratings yet
- 5fc56cb37a6847288b78b547 - Using Kobo ToolboxDocument4 pages5fc56cb37a6847288b78b547 - Using Kobo Toolboxpouya rahmanyNo ratings yet
- Company Profile ASIA ONE - 2022Document15 pagesCompany Profile ASIA ONE - 2022Nur SiswantoNo ratings yet
- Process Payments & ReceiptsDocument12 pagesProcess Payments & ReceiptsAnne FrondaNo ratings yet
- Cleaning Validation Master Plan PDFDocument9 pagesCleaning Validation Master Plan PDFBREWSKINo ratings yet
- CH9-Diversification and AcquisitionsDocument9 pagesCH9-Diversification and AcquisitionsVincent LeruthNo ratings yet
- Salary Income Tax Calculation in EthiopiaDocument4 pagesSalary Income Tax Calculation in EthiopiaMulatu Teshome95% (37)
- Dynamic Bearing Capacity of Shallow FoundationDocument31 pagesDynamic Bearing Capacity of Shallow FoundationLingeswarran NumbikannuNo ratings yet