You might also like
- Reverse and Prevent Heart Disease: Natural Ways to Stop and Prevent Heart Disease, Using Plant-Based Oil-Free Diets (Cure Congestive Heart Failure)From EverandReverse and Prevent Heart Disease: Natural Ways to Stop and Prevent Heart Disease, Using Plant-Based Oil-Free Diets (Cure Congestive Heart Failure)No ratings yet
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- NBME 7 KeyDocument6 pagesNBME 7 KeyQaim ShahNo ratings yet
- Types of Cardiovascular Disease in The HeartDocument7 pagesTypes of Cardiovascular Disease in The Heartissey1652No ratings yet
- (Ebook) Hansen, Richard A. - Get Well at Home (Natural Healing Remedies, Cancer, Heart Disease, Arthritis, More!)Document442 pages(Ebook) Hansen, Richard A. - Get Well at Home (Natural Healing Remedies, Cancer, Heart Disease, Arthritis, More!)popovicedo100% (5)
- Cardiac PathophysiologyDocument36 pagesCardiac Pathophysiologykim suhoNo ratings yet
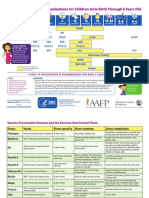
- Parent Ver SCH 0 6yrs AafpDocument2 pagesParent Ver SCH 0 6yrs AafpcicitNo ratings yet
- BORLAND Douglas Infuluenza PDFDocument18 pagesBORLAND Douglas Infuluenza PDFJxson GomezNo ratings yet
- Angina Pectoris, (Heart Chest Pain) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAngina Pectoris, (Heart Chest Pain) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Rheumatic Heart DiseaseDocument10 pagesRheumatic Heart DiseaseSuhas IngaleNo ratings yet
- Swine Diagnostic Manual 4thedDocument44 pagesSwine Diagnostic Manual 4thedthanh ba matNo ratings yet
- What Is Angina?Document30 pagesWhat Is Angina?Bentoys Street100% (1)
- Pedia TicklersDocument24 pagesPedia Ticklersjoshua espirituNo ratings yet
- Angina PectorisDocument6 pagesAngina PectorisMaricel LabiranNo ratings yet
- Coronary Artery Disease Symptoms: CholesterolDocument21 pagesCoronary Artery Disease Symptoms: CholesterolLau AngelNo ratings yet
- Angina Pectoris OverviewDocument6 pagesAngina Pectoris OverviewClarisse GomosNo ratings yet
- Heart DiseaseDocument11 pagesHeart DiseaseSohel BangiNo ratings yet
- Rheumatic Heart DiseaseDocument3 pagesRheumatic Heart DiseaseSachin DwivediNo ratings yet
- Respiratory System DiseasesDocument6 pagesRespiratory System DiseasesWheya OliverosNo ratings yet
- Angina PectorisDocument7 pagesAngina PectorisMovie Clips InternationalNo ratings yet
- Management & Nursing Care of Patient With Coronary Artery DiseasesDocument49 pagesManagement & Nursing Care of Patient With Coronary Artery DiseasesSamah AdnanNo ratings yet
- Cardiovascular DiseaseDocument73 pagesCardiovascular DiseaseAli SherNo ratings yet
- Toate Bolile CardiovasculareDocument6 pagesToate Bolile CardiovasculareAnca CopreanNo ratings yet
- Management Nursing CareDocument49 pagesManagement Nursing CareShreya SinhaNo ratings yet
- 3 Chest Discomfort KuliahDocument29 pages3 Chest Discomfort KuliahRoby KieranNo ratings yet
- Possible Causes of Chest PainDocument4 pagesPossible Causes of Chest PainironNo ratings yet
- Angina PectorisDocument13 pagesAngina Pectorisgreathari1998No ratings yet
- AnginaPectoris 1 PDFDocument2 pagesAnginaPectoris 1 PDFndre_bocchaanNo ratings yet
- Management & Nursing Care of Patient With Coronary Artery DiseasesDocument49 pagesManagement & Nursing Care of Patient With Coronary Artery DiseaseslouradelNo ratings yet
- Diseases of Circulatory System: ScienceDocument3 pagesDiseases of Circulatory System: ScienceAngelieV.RemediosNo ratings yet
- Angina Pectoris: Chest Pain Caused by Coronary Artery ObstructionDocument3 pagesAngina Pectoris: Chest Pain Caused by Coronary Artery Obstructionjama jamsNo ratings yet
- Pathophysiology of Angina Pectoris: Reported By: Maryross M. EspuertaDocument10 pagesPathophysiology of Angina Pectoris: Reported By: Maryross M. Espuertajoyrena ochondraNo ratings yet
- Definitions: By: Saiyed Falakaara Anand Pharmacy CollegeDocument10 pagesDefinitions: By: Saiyed Falakaara Anand Pharmacy CollegeFalak AaraNo ratings yet
- Science Project 2022Document4 pagesScience Project 2022YASHIKA ARORANo ratings yet
- Angina PectorisDocument8 pagesAngina PectorisRia BunagNo ratings yet
- Introduction - MIDocument10 pagesIntroduction - MIkhimiiiNo ratings yet
- How The Heart WorksDocument11 pagesHow The Heart Worksprasanta_bbsrNo ratings yet
- Heart Attack (Myocardial Infarction) : Chest PainDocument11 pagesHeart Attack (Myocardial Infarction) : Chest PainAmitza AmeliaNo ratings yet
- Angina PectorisDocument3 pagesAngina PectorisputrijauharigayatrieNo ratings yet
- Heart Attack (Myocardial Infection)Document3 pagesHeart Attack (Myocardial Infection)mbok diyirNo ratings yet
- Angina PectorisDocument20 pagesAngina PectorisJyoti singhNo ratings yet
- Adoptante-Myocardial Infarction ReportDocument27 pagesAdoptante-Myocardial Infarction Reportjoyrena ochondraNo ratings yet
- Heart AttackDocument12 pagesHeart AttackPaul NeedhamNo ratings yet
- LO Dan WO Cardio Week 4 (Jumat)Document38 pagesLO Dan WO Cardio Week 4 (Jumat)Alan Dwi SetiawanNo ratings yet
- Stroke - MPharm - HHMDocument52 pagesStroke - MPharm - HHMIsrat Jahan Surovy 2225400672No ratings yet
- Ischemic Cardiac Conditions Cardiac Muscle Dysfunction: Dr. Afaq Ahmad PT Cardiopulmonary Physical TherapyDocument19 pagesIschemic Cardiac Conditions Cardiac Muscle Dysfunction: Dr. Afaq Ahmad PT Cardiopulmonary Physical TherapyHUSNAIN TECH AND FUNNo ratings yet
- Angina PectorisDocument1 pageAngina PectorisVivien IgnacioNo ratings yet
- 0 No Musc. Contrac'n, 1-Visible Musc. Con W/no or Trace Movement, 2-Limb Movmnt But Not AgaistDocument7 pages0 No Musc. Contrac'n, 1-Visible Musc. Con W/no or Trace Movement, 2-Limb Movmnt But Not AgaistGirlie TeruelNo ratings yet
- Heart Disease: Symptoms of Heart Disease in Your Blood Vessels (Atherosclerotic Disease)Document22 pagesHeart Disease: Symptoms of Heart Disease in Your Blood Vessels (Atherosclerotic Disease)Kenneth Jay EdnacoNo ratings yet
- Cardio Vascular SystemDocument19 pagesCardio Vascular SystemÑaazir ŘomiőNo ratings yet
- By Mayo Clinic StaffDocument7 pagesBy Mayo Clinic StaffKeith PerryNo ratings yet
- Chest PainDocument24 pagesChest Painjawad_ahmedNo ratings yet
- Proper Way To Maintain A Healthy Circulatory and Respiratory SystemDocument4 pagesProper Way To Maintain A Healthy Circulatory and Respiratory SystemJakob IsraelNo ratings yet
- 2 Days Training Module 2.Document25 pages2 Days Training Module 2.ArumNo ratings yet
- LP UapDocument18 pagesLP UapHat MutisalNo ratings yet
- 6th Chapter DDDocument225 pages6th Chapter DDRameen RizviNo ratings yet
- Symptoms: Heart DiseaseDocument4 pagesSymptoms: Heart DiseaseCharlene Mae B. OrdonioNo ratings yet
- Vascular SurgeryDocument96 pagesVascular SurgeryHiritk RoshanNo ratings yet
- Ischemic Heart DiseaseDocument24 pagesIschemic Heart DiseaseMartha ChaseNo ratings yet
- Angina 2Document3 pagesAngina 2Afdol Triatmojo SikumbangNo ratings yet
- Coronary Artery DiseaseDocument15 pagesCoronary Artery DiseaseMuhammad Daha SanusiNo ratings yet
- Bio Investigatory ProjectDocument20 pagesBio Investigatory ProjectMariaNo ratings yet
- ANGINADocument24 pagesANGINAArya GaunkerNo ratings yet
- By Mayo Clinic Staff: Characteristics of Stable AnginaDocument8 pagesBy Mayo Clinic Staff: Characteristics of Stable AnginaDarryl SpencerNo ratings yet
- What Is Cardiovascular DiseaseDocument84 pagesWhat Is Cardiovascular DiseaseNovelyn PuaNo ratings yet
- Pathogenic BacteriaDocument6 pagesPathogenic BacteriaNit ZeNo ratings yet
- Dr. Noto ID HandoutDocument35 pagesDr. Noto ID HandoutSoleil DaddouNo ratings yet
- The Treatment of Cattle by Homeopathy - Macleod, GeorgeDocument118 pagesThe Treatment of Cattle by Homeopathy - Macleod, Georgerjkl6No ratings yet
- 52 Q. Medicine 2nd Half PDFDocument15 pages52 Q. Medicine 2nd Half PDFFahad2036No ratings yet
- IMCI Chart 2014 EditionDocument80 pagesIMCI Chart 2014 EditionHarold DiasanaNo ratings yet
- ICU-Acquired Infections in Immunocompromised PatientsDocument18 pagesICU-Acquired Infections in Immunocompromised Patientsdarkangelmx1No ratings yet
- Daftar Isi Paediatrica IndonesianaDocument16 pagesDaftar Isi Paediatrica IndonesianaYURIS WIRDANo ratings yet
- Asthma Bronchiolitis P Nemo NiaDocument64 pagesAsthma Bronchiolitis P Nemo NiainyesuaNo ratings yet
- Module 2Document29 pagesModule 2Melody SorianoNo ratings yet
- Study Guide No 5 - Paolo o JavierDocument30 pagesStudy Guide No 5 - Paolo o JavierlordonorNo ratings yet
- Treatment and Prognosis of Common Variable ImmunodeficiencyDocument11 pagesTreatment and Prognosis of Common Variable ImmunodeficiencyJoaoNo ratings yet
- No. Nama Penyakit Kode Dan Nama Kode Diagnosa ICD 10Document21 pagesNo. Nama Penyakit Kode Dan Nama Kode Diagnosa ICD 10Chaqhim YvciNo ratings yet
- English Form 1 - Question PaperDocument9 pagesEnglish Form 1 - Question PaperFredrick LangatNo ratings yet
- Hydrocarbon PoisoningDocument10 pagesHydrocarbon PoisoningVarshith GandlaNo ratings yet
- Abbreviated PI ABBOTIC DraftDocument2 pagesAbbreviated PI ABBOTIC Draftadani 2372No ratings yet
- Case Study,,,,,,pneumoniaDocument52 pagesCase Study,,,,,,pneumoniaJaillah Reigne Cura0% (1)
- Drug StudyDocument12 pagesDrug StudyHannah DuyagNo ratings yet
- Ecografia Toracica PDFDocument12 pagesEcografia Toracica PDFCristinaLucanNo ratings yet
- Concept Map Complex Care 2017Document7 pagesConcept Map Complex Care 2017api-401537905No ratings yet
- 12 STEM C - CASIÑO - Assignment 2.3.1Document4 pages12 STEM C - CASIÑO - Assignment 2.3.1CASIÑO SHANE VAST ANDREINo ratings yet
- Vaccines CircaDocument10 pagesVaccines CircamariavillaresNo ratings yet
- Health Care-Associated Infections - Best PracticesDocument9 pagesHealth Care-Associated Infections - Best PracticesJoshua DiaoNo ratings yet
- Paediatrics SbaDocument34 pagesPaediatrics SbaAhmad Syahmi YZ100% (1)
- HOSPITAL Data Dictionary35Document102 pagesHOSPITAL Data Dictionary35a8m1i2r3No ratings yet