0% found this document useful (0 votes)
501 views1 pageData Privacy Request Form Template
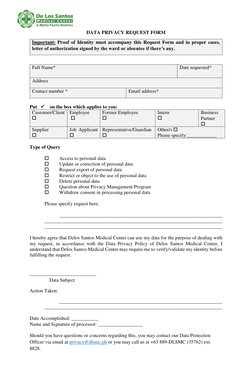
This document is a data privacy request form for Delos Santos Medical Center. It requests the individual's name, address, contact information, and relationship to the organization. The individual must select the type of data privacy request, such as accessing, updating, deleting personal data. The individual consents to the organization using their data to process the request according to the organization's data privacy policy. The organization may require identity verification before fulfilling the request.
Uploaded by
qwertyuiopkmrrCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
501 views1 pageData Privacy Request Form Template
This document is a data privacy request form for Delos Santos Medical Center. It requests the individual's name, address, contact information, and relationship to the organization. The individual must select the type of data privacy request, such as accessing, updating, deleting personal data. The individual consents to the organization using their data to process the request according to the organization's data privacy policy. The organization may require identity verification before fulfilling the request.
Uploaded by
qwertyuiopkmrrCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd
- Data Privacy Request Form