You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Solution Manual For Engineering Mechanics Statics and Dynamics 2nd Edition by PleshaDocument376 pagesSolution Manual For Engineering Mechanics Statics and Dynamics 2nd Edition by PleshaVenkat Dalai0% (5)
- Free Sheet Music For Band Song For Peace SCOREDocument18 pagesFree Sheet Music For Band Song For Peace SCORESergio Moles SamperNo ratings yet
- Synopsis of Training and Development AjayDocument19 pagesSynopsis of Training and Development Ajayajaykaransingh100% (2)
- Task1 LettersDocument98 pagesTask1 Lettersrak.cea4098100% (1)
- ITChennaiDocument219 pagesITChennaiDhananjayan GopinathanNo ratings yet
- Wind Tunnel ProposalDocument7 pagesWind Tunnel Proposalapi-3748560100% (4)
- Biology Life On Earth 10Th Edition Audesirk Test Bank Full Chapter PDFDocument48 pagesBiology Life On Earth 10Th Edition Audesirk Test Bank Full Chapter PDFodetteisoldedfe100% (14)
- RXII Series User ManualDocument220 pagesRXII Series User ManualDavid DuarteNo ratings yet
- 5S-Checklist Akro MillsDocument1 page5S-Checklist Akro MillsPankaj GarodeNo ratings yet
- File DelDocument48 pagesFile DelYeremiaNo ratings yet
- Introducing Financial Derivatives - ScribdDocument18 pagesIntroducing Financial Derivatives - ScribdVipul MehtaNo ratings yet
- Red, Amber and Green List Rules For Entering England - GOV - UKDocument7 pagesRed, Amber and Green List Rules For Entering England - GOV - UKMohammed SulimanNo ratings yet
- Eur - Cover/Bosch Fl./conical 1:8 Gr.I: Gear Pumps Group I LeftDocument2 pagesEur - Cover/Bosch Fl./conical 1:8 Gr.I: Gear Pumps Group I LeftTadas PNo ratings yet
- HLTH635 SyllabusDocument6 pagesHLTH635 SyllabusEshany EdwardsNo ratings yet
- Rubber Base: School of Mechanical EngineeringDocument1 pageRubber Base: School of Mechanical EngineeringMUHAMMAD ALIIF MOHD ZAKINo ratings yet
- The Science: Orbital Mechanics: Kepler's Laws of Planetary MotionDocument7 pagesThe Science: Orbital Mechanics: Kepler's Laws of Planetary MotionDeeksha TripathiNo ratings yet
- Communication Skills ExamDocument33 pagesCommunication Skills Exammalware100% (1)
- Financial Statement AnalysisDocument6 pagesFinancial Statement AnalysisCIPRIANO, Rodielyn L.No ratings yet
- Power Plant Off-Grid PDFDocument5 pagesPower Plant Off-Grid PDFmak makNo ratings yet
- Golden Rules of User InterfaceDocument3 pagesGolden Rules of User InterfaceVijaya AlukapellyNo ratings yet
- Laureen Odendo Mba 2018Document84 pagesLaureen Odendo Mba 2018Maria HauleNo ratings yet
- Gatekeeper Complete Contract Management Template 2021Document41 pagesGatekeeper Complete Contract Management Template 2021Chirec LegalNo ratings yet
- Rising Damp - FactsheetDocument2 pagesRising Damp - FactsheetAdam ClutterbuckNo ratings yet
- Dispa, DRRM Assests Inventory - Encoding TemplateDocument15 pagesDispa, DRRM Assests Inventory - Encoding TemplateBRGY SEVENONEPAYBNo ratings yet
- Updates On The Treatment of Pterygium: Serbian Journal of Experimental and Clinical Research September 2016Document7 pagesUpdates On The Treatment of Pterygium: Serbian Journal of Experimental and Clinical Research September 2016Arfadin YusufNo ratings yet
- Microfossils Description Paper: Palaeontology Practical: KalpanadekakalitaDocument32 pagesMicrofossils Description Paper: Palaeontology Practical: Kalpanadekakalitarikalave ramanNo ratings yet
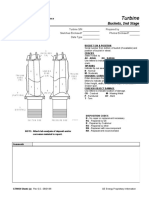
- Turbine: Buckets, 2nd StageDocument2 pagesTurbine: Buckets, 2nd StagejhonnattanrvNo ratings yet
- Centennial IPADocument1 pageCentennial IPAHari RNo ratings yet
- Theme of MusicDocument11 pagesTheme of MusicBarathyNo ratings yet
- A Study On Mutual Fund and Awareness of Mutual Fund Among Insurance AdvisorDocument6 pagesA Study On Mutual Fund and Awareness of Mutual Fund Among Insurance AdvisorRichard SinghNo ratings yet