You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Surely Youre Joking MR Feynman Adventures of A CuDocument2 pagesSurely Youre Joking MR Feynman Adventures of A CuCatalinTdr13% (8)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- 4.1 Genetic Counselling 222Document12 pages4.1 Genetic Counselling 222Sahar JoshNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Ginecologia Women's Imaging Obstetrics and GynecologyDocument199 pagesGinecologia Women's Imaging Obstetrics and GynecologyAnca LoyolaNo ratings yet
- Tietz Fundamentals of Clinical Chemistry and Molecular Diagnostics e Book 8th Edition Ebook PDF VersionDocument62 pagesTietz Fundamentals of Clinical Chemistry and Molecular Diagnostics e Book 8th Edition Ebook PDF Versionjack.murgia17597% (36)
- FIGO Accreta Prenantal DiagnosisDocument7 pagesFIGO Accreta Prenantal DiagnosisYosef Dwi Cahyadi SalanNo ratings yet
- Hartmann's Procedure: Patient Information - General SurgeryDocument7 pagesHartmann's Procedure: Patient Information - General SurgeryputriNo ratings yet
- New Inborn Error of MetabolismDocument45 pagesNew Inborn Error of Metabolismmannan mangal100% (1)
- Acog Gestacion Multiple 2016 PDFDocument16 pagesAcog Gestacion Multiple 2016 PDFRicardo QuintanaNo ratings yet
- Chole Doc Hal Cysts Diagnosis and TreatmentDocument16 pagesChole Doc Hal Cysts Diagnosis and TreatmentputriNo ratings yet
- Jurnal Radio 2 PDFDocument20 pagesJurnal Radio 2 PDFnadiabella_No ratings yet
- Ecr2011 C-1333Document15 pagesEcr2011 C-1333putriNo ratings yet
- DAFPUSDocument9 pagesDAFPUSputriNo ratings yet
- DAFPUSDocument9 pagesDAFPUSputriNo ratings yet
- CHRISMEDJHealthRes52165-7285991 201419Document2 pagesCHRISMEDJHealthRes52165-7285991 201419putriNo ratings yet
- Daftar PustakaDocument6 pagesDaftar PustakaputriNo ratings yet
- 6182783Document9 pages6182783putriNo ratings yet
- Radial RayDocument8 pagesRadial RayputriNo ratings yet
- Pulmonary Edema Vs PneumoniaDocument59 pagesPulmonary Edema Vs PneumoniaInstalasi RadiologiNo ratings yet
- DDocument10 pagesDputriNo ratings yet
- DDocument10 pagesDputriNo ratings yet
- OkDocument4 pagesOkputriNo ratings yet
- Review - The Exstrophy-Epispadias Complex PDFDocument17 pagesReview - The Exstrophy-Epispadias Complex PDFluqmanhasansNo ratings yet
- BacaDocument5 pagesBacaputriNo ratings yet
- GR Up: SM Journal of Pediatric SurgeryDocument3 pagesGR Up: SM Journal of Pediatric SurgeryputriNo ratings yet
- Ruang IGDDocument40 pagesRuang IGDputriNo ratings yet
- Morning Report: KAMIS, 31 Januari 2019 Konsulen: DR - Dr.elysanti Dwi Martadiani, SP - Rad (K) Residen: DR - Widyasari, DR - YanDocument2 pagesMorning Report: KAMIS, 31 Januari 2019 Konsulen: DR - Dr.elysanti Dwi Martadiani, SP - Rad (K) Residen: DR - Widyasari, DR - YanputriNo ratings yet
- Morning Report - OaDocument5 pagesMorning Report - OaputriNo ratings yet
- Respiratory Status of Darkroom Technicians Working in Various Radiology Departments in Harare, ZimbabweDocument11 pagesRespiratory Status of Darkroom Technicians Working in Various Radiology Departments in Harare, ZimbabweputriNo ratings yet
- Tadesse 352014 IJMPCR15916Document5 pagesTadesse 352014 IJMPCR15916putriNo ratings yet
- Hirscprung 2 PDFDocument5 pagesHirscprung 2 PDFputriNo ratings yet
- Evaluating Cardiomegaly by Radiological Cardiothoracic Ratio As Compared To Conventional EchocardiographyDocument3 pagesEvaluating Cardiomegaly by Radiological Cardiothoracic Ratio As Compared To Conventional EchocardiographyputriNo ratings yet
- Seminar HBOT Bali OKT 2017 PDFDocument32 pagesSeminar HBOT Bali OKT 2017 PDFputriNo ratings yet
- Proposal Seminar Revisi 1Document3 pagesProposal Seminar Revisi 1putriNo ratings yet
- Review JurnalDocument4 pagesReview JurnalprabuNo ratings yet
- Iranjradiol 12 02 12451 PDFDocument5 pagesIranjradiol 12 02 12451 PDFNovia RambakNo ratings yet
- Human Heredity Principles and Issues 11Th Edition Cummings Test Bank Full Chapter PDFDocument24 pagesHuman Heredity Principles and Issues 11Th Edition Cummings Test Bank Full Chapter PDFAshleyMaciasowbj100% (8)
- Antenatal ScreeningDocument5 pagesAntenatal ScreeningShahzaib Ali100% (1)
- Chromosomal Aberrations Just in CaseDocument8 pagesChromosomal Aberrations Just in CaseJahn Alaina DadoNo ratings yet
- 7 - Ethical Issues in Pre-Natal DiagnosisDocument12 pages7 - Ethical Issues in Pre-Natal DiagnosisMohammed HussienNo ratings yet
- Anencephaly and EncephaloceleDocument14 pagesAnencephaly and EncephaloceleleaslimNo ratings yet
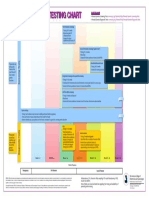
- Prenatal Genetic Testing ChartDocument1 pagePrenatal Genetic Testing ChartMorningDewNo ratings yet
- Obg Procedures FinalDocument60 pagesObg Procedures FinalVeena DalmeidaNo ratings yet
- Final NPRD, 2021Document28 pagesFinal NPRD, 2021Maruthi RoshanNo ratings yet
- Contemporary Maternal Newborn Nursing 9th Edition Test BankDocument34 pagesContemporary Maternal Newborn Nursing 9th Edition Test BankCharlotte Reddy100% (36)
- Normal and Abnormal Early PregnancyDocument30 pagesNormal and Abnormal Early PregnancyKhrisna AdjiNo ratings yet
- Gendia Brochure NIPTDocument4 pagesGendia Brochure NIPTrajeshbhramaNo ratings yet
- Nanda-2019-The Obstetrician & GynaecologistDocument2 pagesNanda-2019-The Obstetrician & GynaecologistrichaNo ratings yet
- Afp20141215p851 PDFDocument8 pagesAfp20141215p851 PDFViviane BarbosaNo ratings yet
- TOG Evolution in Screening For Down SyndromeDocument7 pagesTOG Evolution in Screening For Down SyndromeMarNo ratings yet
- Essentials of Human Development A Life Span View 1st Edition Kail Test BankDocument33 pagesEssentials of Human Development A Life Span View 1st Edition Kail Test BankRobertYangfmspj100% (20)
- Care of Mother and Child at Risk or With Problems - Acute and Chronic (Lecture)Document97 pagesCare of Mother and Child at Risk or With Problems - Acute and Chronic (Lecture)Mariah Alexis EncinaNo ratings yet
- Validation of The Placenta Accreta Index (PAI) - Improving The Antenatal Diagnosis of The Morbidly Adherent PlacentaDocument2 pagesValidation of The Placenta Accreta Index (PAI) - Improving The Antenatal Diagnosis of The Morbidly Adherent PlacentaOmpNo ratings yet
- Nihms 1590580Document29 pagesNihms 1590580patricia brucellariaNo ratings yet
- Perinatal Palliative, Too Early, Too Late?Document39 pagesPerinatal Palliative, Too Early, Too Late?Dewi Wara ShintaNo ratings yet
- Session 20Document2 pagesSession 20Bernadeth Barrientos ZamoraNo ratings yet
- Maternity Information BookletDocument114 pagesMaternity Information BookletDeirdre BrennanNo ratings yet
- Obstetrics - Topical Past Papers (2007-2019)Document32 pagesObstetrics - Topical Past Papers (2007-2019)Humna YounisNo ratings yet
- Abnormal Meiosis And/or FertilizationDocument6 pagesAbnormal Meiosis And/or FertilizationSia BhatiaNo ratings yet