You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5811)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Joel Paris-The Intelligent Clinician's Guide To The DSM-5®-Oxford University Press (2013)Document265 pagesJoel Paris-The Intelligent Clinician's Guide To The DSM-5®-Oxford University Press (2013)JC Barrientos100% (8)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- MUST To KNOW in HematologyDocument46 pagesMUST To KNOW in HematologyRona Salando100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Acute Stress DisorderDocument17 pagesAcute Stress DisorderdemocratieivanNo ratings yet
- Wound Care NursingDocument94 pagesWound Care Nursingapi-236188238No ratings yet
- PsychoeducationDocument9 pagesPsychoeducationSrinivas Pandeshwar100% (1)
- SLE Made EasyDocument482 pagesSLE Made EasySumayyia Qamar100% (1)
- Odd Exercises For Physical VigorDocument19 pagesOdd Exercises For Physical VigorKristijan Kostić100% (1)
- Bruising OSCE History Taking PaediatricsDocument6 pagesBruising OSCE History Taking PaediatricsJJ LimNo ratings yet
- Boala PakinsonDocument120 pagesBoala PakinsonMadalina CordonasuNo ratings yet
- HS 25 Literary AnalysisDocument11 pagesHS 25 Literary AnalysisChelsea Reyna TolentinoNo ratings yet
- Sample Letter of SupportDocument2 pagesSample Letter of SupportZuardin ArifNo ratings yet
- Consumers' Perception of Beef Burgers With Different Healthy Attributes PDFDocument21 pagesConsumers' Perception of Beef Burgers With Different Healthy Attributes PDFZuardin ArifNo ratings yet
- Odonto: Forensic TestDocument1 pageOdonto: Forensic TestZuardin ArifNo ratings yet
- Indian Council For Cultural Relations: Scholarships For Foreign NationalsDocument23 pagesIndian Council For Cultural Relations: Scholarships For Foreign NationalsZuardin ArifNo ratings yet
- DD Indonesia JermanDocument1 pageDD Indonesia JermanZuardin ArifNo ratings yet
- Koding Rawat InapDocument38 pagesKoding Rawat InapWidya OktarinaNo ratings yet
- 2016 Ramos Inpact Feeling MehDocument4 pages2016 Ramos Inpact Feeling MehPaula Glenda Ferrer - Program ChairNo ratings yet
- JMI MPT Entrance Paper 2024Document15 pagesJMI MPT Entrance Paper 2024Harshita bansalNo ratings yet
- Dengue Hemorrhagic FeverDocument33 pagesDengue Hemorrhagic FeverCharlz ZipaganNo ratings yet
- 15 Ways To Get Rid of Stammering Exercises, Treatment, Home CuresDocument14 pages15 Ways To Get Rid of Stammering Exercises, Treatment, Home CuresJames Diego HayesNo ratings yet
- Revival, Modernization and Integration of Indian Traditional Herbal Medicine in Clinical Practice: Importance, Challenges and FutureDocument11 pagesRevival, Modernization and Integration of Indian Traditional Herbal Medicine in Clinical Practice: Importance, Challenges and FutureRigotti BrNo ratings yet
- My Courses: Home Baed-Pdev2111-2012S Week 9: Mental Health and Well-Being in Middle and Late Adolescence (2) Writtenwork2Document7 pagesMy Courses: Home Baed-Pdev2111-2012S Week 9: Mental Health and Well-Being in Middle and Late Adolescence (2) Writtenwork2Nicole TenoriaNo ratings yet
- Digestive System 1Document35 pagesDigestive System 1Anthony LopezNo ratings yet
- Administering Metoprolol IV Push 1Document22 pagesAdministering Metoprolol IV Push 1api-357388170No ratings yet
- The Big Family Day OutDocument2 pagesThe Big Family Day OutPlimmerton Residents' AssociationNo ratings yet
- Efek Eating Disorder Terhadap Remaja: Nindy Sabrina, S.GZ, M.SCDocument22 pagesEfek Eating Disorder Terhadap Remaja: Nindy Sabrina, S.GZ, M.SClulukNo ratings yet
- Revision MCQsDocument6 pagesRevision MCQswiamNo ratings yet
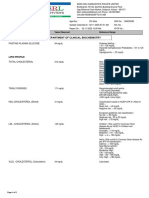
- Department of Clinical Biochemistry: Fasting Plasma GlucoseDocument2 pagesDepartment of Clinical Biochemistry: Fasting Plasma Glucosearavind sNo ratings yet
- Emetophobia: A Fear of Vomiting: Abhijeet D. Faye, Sushil Gawande, Rahul Tadke, Vivek C. Kirpekar, Sudhir H. BhaveDocument3 pagesEmetophobia: A Fear of Vomiting: Abhijeet D. Faye, Sushil Gawande, Rahul Tadke, Vivek C. Kirpekar, Sudhir H. Bhavejayadevan vkNo ratings yet
- Eczema DR Ahmed KamelDocument52 pagesEczema DR Ahmed KamelMostafa EidNo ratings yet
- Mental Health Nursing.: Lesson 1Document177 pagesMental Health Nursing.: Lesson 1Eng Steve WairuaNo ratings yet
- Etiologic FactorsDocument1 pageEtiologic FactorsMARIA CHARMIN M. MEJIANo ratings yet
- Cardiac Tamponade: Squeezing The Heart Until It StopsDocument4 pagesCardiac Tamponade: Squeezing The Heart Until It StopsJesse FlingNo ratings yet
- Articulo de e Coli en InglesDocument3 pagesArticulo de e Coli en Inglesjuan gonzalezNo ratings yet