Professional Documents
Culture Documents
El Gran Escape
Uploaded by
PoPe MendeleroCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
El Gran Escape
Uploaded by
PoPe MendeleroCopyright:
Available Formats
Downloaded from www.ajronline.org by 89.130.189.147 on 03/15/18 from IP address 89.130.189.147. Copyright ARRS.
For personal use only; all rights reserved
Perspective
The Great Escape: Interfascial Decompression Planes of the
Retroperitoneum
Richard M. Gore 1, Dennis M. Balfe 2, Robert I. Aizenstein 3, Paul M. Silverman 4
R etroperitoneal fluid collections re- layers representing fused leaves of apposed plane [10, 11]. This potential space may be re-
sult from a variety of infectious, embryonic mesentery [6–8] (Fig. 1 and Ap- cruited for the decompression of fluid collec-
neoplastic, inflammatory, and trau- pendix). The primary body wall, which is the tions arising in either of the spaces it bounds.
matic causes. In most instances, these fluid outermost layer of the embryo, is formed by The perinephric space is divided by thin
collections remain in their compartment of ori- mesenchyme, which develops in the vertebral fibrous lamellae (Fig. 2) into multiple com-
gin confined by the anterior and posterior renal bodies, paraspinal muscles, and the psoas partments that may or may not communicate
fascia, lateroconal fascia, adhesions, or inflam- muscle. The body wall is lined with transver- [12]. These fibrous lamellae also form bridg-
matory closure of potential outlets [1, 2]. How- salis fascia, which forms the outer border of ing septa that traverse the perinephric fat and
ever, when large volumes of fluid develop the retroperitoneal and peritoneal cavities. interconnect the renal capsule and anterior
rapidly, the capacity of the retroperitoneal Deep in relation to the transversalis fascia lies and posterior renal fasciae. These bridging
space of origin to accommodate the fluid may a variable amount of properitoneal fat that septa are continuous with the anterior and
be overwhelmed, often causing the recruit- forms the posterior pararenal space. This posterior interfascial planes and may serve as
ment of laminated, variably fused, and poten- small, almost unoccupied space is seldom the a bidirectional conduit for the spread of
tial expansile retroperitoneal fascial planes for primary site of abnormality. Two fat pads ex- blood, fluid, edema, and infiltrating soft tis-
decompression [3–5]. These fascial planes also ist in this space: one lies posterolateral and sue from the perirenal interfascial planes into
serve as a conduit for the spread of fluid, in- one directly ventral to the quadratus lumbo- the perinephric space.
flammation, and tumor. This perspective ana- rum muscle [9]. The next embryologic development key to
lyzes recent concepts concerning the origin, The kidneys form in the pelvis in early em- this discussion is the rotation and subsequent
location, nature, and significance of fascial bryologic life and then ascend to their adult fusion of the gut and its dorsal mesentery. In
planes and their ability to serve as spaces that position. As a result, the fascia that surrounds this complex process, the mesentery, which
can decompress retroperitoneal fluid collec- each kidney forms a long tapered cone that contains the pancreas and duodenum, rotates
tions and infiltrating diseases. fuses at its posterior and lateral aspects to the and fuses. Under the influence of the rapidly
surface of the properitoneal fat. At this point of growing liver, the stomach and duodenum are
development, two defined retroperitoneal rotated counterclockwise, so that the left side
Embryologic Considerations spaces exist: the perirenal space, which con- of this mesentery becomes anterior. The right
An understanding of the distribution of tains the kidneys, adrenal glands, proximal side of the mesentery becomes closely ap-
fluid in the retroperitoneum is contingent on ureters, and fat; and the posterior pararenal posed to the body wall, aorta, inferior vena
an appreciation of the fact that the retroperi- space, which contains only fat. A potential cava, and anterior part of the right renal fascia.
toneum forms in layers and that the retroperi- space is also created between these fused sur- In fusing, the dorsal mesoduodenum forms the
toneal fascia is composed of multiple discrete faces, the posterior interfascial or retrorenal pancreaticoduodenal space, creating another
Received December 9, 1999; accepted after revision January 24, 2000.
1
Department of Radiology, Evanston Hospital–Northwestern University, 2650 Ridge Ave., Evanston, IL 60201. Address correspondence to R. M. Gore.
2
Department of Diagnostic Radiology, Mallinckrodt Institute of Radiology, Washington University School of Medicine, 510 S. Kingshighway, St. Louis, MO 63110.
3
Department of Radiology, University of Illinois Medical Center, 1740 W. Taylor, Chicago, IL 60612.
4
Department of Radiology, M. D. Anderson Cancer Center, Department of Radiology, Box 057, 1515 Holcomb Blvd., Houston, TX 77030.
AJR 2000;175:363–370 0361–803X/00/1752–363 © American Roentgen Ray Society
AJR:175, August 2000 363
Fig. 1.—Retroperitoneal
Gore et al. and interfascial planes. Drawing at level of renal hila shows that
renal and lateroconal fasciae are laminated planes composed of apposed layers of embry-
onic mesentery. Thickness of interfascial planes is exaggerated to illustrate their poten-
tially expansile nature. Note that perinephric spaces (PRS) are closed medially.
Retromesenteric space is continuous across midline. Retromesenteric anterior interfas-
cial space (RMP), retrorenal posterior interfascial space (RRS), and lateroconal plane
communicate at fascial trifurcation (arrows). A = aorta, APS = anterior pararenal space,
ARF = anterior renal fascia, DPS = dorsal pleural sinus, IVC = inferior vena cava, LCF = lat-
eroconal fascia, PP = parietal peritoneum, PPS = posterior pararenal space, PRF = poste-
rior renal fascia, TF = transversalis fascia, asterisk = posterior peritoneal recess.
(Reprinted from [3])
Downloaded from www.ajronline.org by 89.130.189.147 on 03/15/18 from IP address 89.130.189.147. Copyright ARRS. For personal use only; all rights reserved
A B
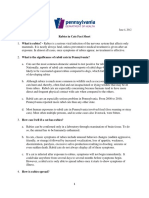
Fig. 2.—Perinephric space bridging septa.
A, Drawing of perinephric space at level of mid pole of kidney shows that perinephric space contains rich
network of bridging septa (open arrows), lymphatics (solid arrow), arteries, and veins (arrowhead). Note
that perirenal lymphatics communicate with small lymph nodes at renal hilum, and that these, in turn, con-
nect with periaortic and pericaval lymph nodes. This lymphatic network provides potential route of spread
for metastatic tumor into perinephric space. (Reprinted from [3])
B and C, T1-weighted (B) and T2-weighted fat-suppressed (C) MR images in 47-year-old man with left-sided
pyelonephritis reveal fluid-filled bridging perinephric septa (arrows).
C
potential space between the fused surfaces of the lateral portions of the anterior pararenal eral in relation to the anterior renal fascia,
these fat-containing structures—an anterior in- space. The mesentery of the descending co- the dorsal mesocolon fuses with the surface
terfascial or retromesenteric plane. lon rotates in a clockwise direction (as of the posterior pararenal fat to form the lat-
Pari passu, the colon and its mesentery un- viewed from below) and its left lateral sur- eroconal fascia. The ascending colon and its
dergo complex rotation and fusion to form face fuses with the anterior renal fascia. Lat- mesentery undergo a 180º counterclockwise
364 AJR:175, August 2000
Interfascial Decompression Planes of the Retroperitoneum
rotation (as viewed from the front) so that its with the pelvic retroperitoneum, interfascial rapidly growing fluid collections may accu-
original left surface faces right. The mesen- fluid collections can spread from the abdomi- mulate is also supported by clinical and imag-
tery of the ascending colon rotates counter- nal retroperitoneum across the midline or into ing observations.
clockwise (as viewed from below) to fuse the pelvis.
with the anterior renal fascia (proximally, be- The concept of recruitable planes sur- Surgical Anatomy
low the transverse duodenum) and distally to rounding the renal fascia can help resolve When performing a right or left hemi-
Downloaded from www.ajronline.org by 89.130.189.147 on 03/15/18 from IP address 89.130.189.147. Copyright ARRS. For personal use only; all rights reserved
fuse with the pancreaticoduodenal space. several conflicting, recently published ca- colectomy, the surgeon mobilizes the as-
The lateral part of the right colon fuses with daver studies that have investigated the ex- cending and descending colons by dissecting
the properitoneal fat to form the lateroconal tension of retroperitoneal fluid into the pelvis through the anterior and lateroconal fusion
fascia. These retromesenteric fusion planes and across midline. Mindell et al. [13], planes beginning at the “white line of Toldt”
create a potential space (the anterior interfas- Kneeland et al. [14], and Mastromatteo et al. [19]. This dissection is usually quite easy,
cial plane) that lies ventral in relation to the [15] have concluded that the cone of the re- nearly bloodless, and does not compromise
anterior renal fascia and dorsal in relation to nal fascia is open, allowing fluid to extend the viability of the bowel, allowing the as-
the mesenteries of the ascending and de- across the midline and into the pelvis [16]. In cending and descending colons to be mobi-
scending colons. two different studies, Raptopoulos et al. [17, lized freely. Similarly, when transabdominal
18] used latex injections of subsequently dis- surgical exposure of either kidney or ureter is
sected cadavers and concluded that the cone required, the procedure is facilitated by the
Anatomic Considerations medial reflection of the overlying colon.
of renal fascia is closed, preventing fluid
The existence of the interfascial retroperi- from crossing the midline and extending into Again, this task is readily accomplished
toneal planes was recently documented in a the pelvis. The interfascial plane concept ac- without the need for sharp dissection. How-
series of cadaveric dissections by Molmenti knowledges that although the renal fascia do ever, these dissecting planes may be difficult
et al. [5]. In that study, latex injected into the indeed form an enclosed space, fluid can leak to develop in patients with a history of pan-
tail of the pancreas entered an anterior inter- through bridging perinephric septa [12] and creatitis [20].
fascial retromesenteric plane that was dorsal extend into the interfascial planes. From
in relation to the anterior pararenal space Anatomic Variants
there, the fascia can descend into the pelvis
and ventral in relation to the anterior renal via the combined interfascial plane and cross The site of fusion between the anterior and
fascia. The plane continued superiorly in re- the midline via the anterior interfascial ret- posterior laminae of the posterior renal fascia
lation to the diaphragm near the esophageal romesenteric plane. normally is lateral in relation to the kidney. If
hiatus; inferiorly in relation to the pelvis this fusion occurs more dorsally than usual,
along the anterolateral surface of the psoas then fluid in the posterior sulcus of the perito-
muscle; and laterally, posteriorly in relation Clinical and Imaging Observations neal cavity can reside in the posterior interfas-
to the descending colon and its mesentery. The concept that the previously described cial retrorenal plane (Fig. 4). Additionally,
This anterior interfascial retromesenteric lines of fusion are expandable planes in which peritoneal fluid can accumulate in the anterior
plane also communicated with the posterior
interfascial retrorenal plane lying between
the posterior renal fascia and the posterior
pararenal space.
The laminated anterior interfascial ret-
romesenteric plane is continuous across the
midline, and it communicates at the fascial
trifurcation (Fig. 3) with the two other po-
tentially expansile planes, the posterior in-
terfascial and lateroconal planes.
In the iliac fossa, the anterior and posterior
renal fascia fuse to form a single multilaminar
fascia, the combined interfascial plane. This
combined interfascial plane continues in the
pelvis along the anterolateral margins of the
psoas muscle contiguous with the pelvic retro-
peritoneal perivesical and presacral spaces.
Therefore, this plane can serve as a decom-
pressing conduit to the pelvis for interfascial
fluid originating in the retroperitoneum. The
inferior blending of Gerota’s fascia also seals
the inferior aspect of the perinephric space.
This prevents the extension of perinephric
fluid from the abdominal retroperitoneum into
Fig. 3.—52-year-old woman with aortic bleeding. CT scan at level of lower poles of kidneys shows hemorrhage
the pelvis. Because the retroperitoneal fascial in anterior interfascial plane (straight open arrow), posterior interfascial plane (curved solid arrow), and latero-
planes traverse the midline and are continuous conal interfascial plane (curved open arrow). These collections meet at fascial trifurcation (straight solid arrow).
AJR:175, August 2000 365
Gore et al.
interfascial retromesenteric planes in patients pararenal space, lesser sac, and subperitoneal teric plane (Fig. 6), or spreading inferiorly in
in whom the mesenteries of the ascending and spaces of the small bowel mesentery and trans- the combined interfascial plane to reach the
descending colons have not completely fused verse mesocolon. In some individuals, fluid pelvic retroperitoneum or superiorly along the
(Fig. 4) to the retroperitoneum. and inflammatory tissue may accumulate in diaphragm to enter the mediastinum.
the retroperitoneal interfascial planes, dissect- Perirenal fluid collections related to pan-
Pancreatitis ing posteriorly (Fig. 5) to involve the posterior creatitis can access the posterior interfascial
Downloaded from www.ajronline.org by 89.130.189.147 on 03/15/18 from IP address 89.130.189.147. Copyright ARRS. For personal use only; all rights reserved
In patients with pancreatitis, inflammatory interfascial retrorenal plane, traversing the plane and extend into the transversalis fascia
fluid most commonly extends into the anterior midline in the anterior interfascial retromesen- through a cleft between the medial border of
Fig. 4.—59-year-old man with fulminant ulcerative
colitis in whom incomplete fusion of fascial planes has
permitted retromesenteric and retrorenal extension of
peritoneal fluid. CT scan shows that ascending (A) and
descending (D) mesocolons have not completely
fused with renal fascia, permitting ascites (straight ar-
rows) to enter anterior interfascial retromesenteric
plane. Posterior renal fascia has also not fused, allow-
ing peritoneal fluid to extend into retrorenal posterior
interfascial planes (curved arrows). These anterior in-
terfascial planes are easily surgically dissected dur-
ing hemicolectomy. Posterior interfascial planes are
readily dissected during nephrectomy.
Fig. 5.—45-year-old woman with interfascial fluid spread in acute pancreatitis Fig. 6.—58-year-old man with pancreatitis and inflammatory fluid spread into interfas-
and retrorenal dissection of fluid in lumbar triangle. Note fluid in left anterior in- cial planes. CT scan shows fluid extending into anterior interfascial space (open
terfascial space (straight open arrow), lateroconal interfascial space (curved arrow), right fascial trifurcation (solid arrow), and subsequently lateroconal and pos-
open arrow), and posterior interfascial space (curved solid arrow). Fluid ex- terior interfascial spaces. Note that fat in anterior pararenal space adjacent to as-
tends to and thickens transversalis fascia (straight solid arrow), dissecting cending colon (AC) is spared.
quadratus lumborum muscles and posterior pararenal fat (arrowhead). This is
source of Grey Turner’s sign of pancreatitis.
366 AJR:175, August 2000
Interfascial Decompression Planes of the Retroperitoneum
the posterior pararenal space and the lateral planes and from there, spread into the peri- 9) are the major causes of duodenal perfora-
border of the quadratus lumborum fat pad, nephric space [12]. tion and the pathologic gas and fluid that
the lumbar triangle. The relatively low posi- may decompress into the anterior interfascial
tion of flank discoloration associated with Urinomas space. Extravasated gas, bile, and pancreatic
pancreatitis (Grey Turner’s sign) is attribut- Encapsulated collections of urine that lie juice may extend into the pancreaticoduode-
able to this lumbar triangle pathway. outside the renal collecting system and ureters nal space and subsequently cross the midline
Downloaded from www.ajronline.org by 89.130.189.147 on 03/15/18 from IP address 89.130.189.147. Copyright ARRS. For personal use only; all rights reserved
most commonly result from obstructive uropa- via the anterior interfascial retromesenteric
Perirenal Hematomas thy and less frequently from abdominal plane. Similar to retroperitoneal fluid, retro-
Subcapsular and perinephric hematomas re- trauma, surgery, or diagnostic instrumentation peritoneal gas readily dissects preestablished
sult from a number of traumatic (biopsy, lithot- [22]. Most urinomas reside in the perinephric interfascial planes (Fig. 10).
ripsy, or blunt abdominal injury) and space. This fluid can access the interfascial
neoplastic (renal cell carcinoma or angiomyo- planes via the bridging perinephric septa or by Colonic Diseases
lipoma) causes [21]. The hematomas can gain direct extension occurring with ureteral disrup- As previously stated, the ascending and
access to the anterior and posterior interfas- tion. Disruption of the ureteropelvic junction descending mesocolons fuse posteriorly with
cial planes via numerous bridging peri- characteristically fills both the anterior and the anterior renal fascia and laterally with the
nephric septa that consist of fibrous lamellae, posterior interfascial planes [23–25] (Fig. 8). anterior surface of the posterior pararenal fat.
which traverse the perirenal space (Fig. 7). Accordingly, the laminated lateroconal and
Conversely, these septa may be a conduit of Duodenal Perforation and Pneumoretroperitoneum anterior interfascial planes partly comprise
hemorrhage or other rapidly accumulating Blunt abdominal trauma, peptic ulcer dis- variably fused layers of mesocolon that have
fluid collections that recruit the interfascial ease, and endoscopic sphincterotomy (Fig. become retroperitoneal. Because the anterior
A B
Fig. 7.—65-year-old man with spontaneous subcapsular renal hemorrhage de-
compressing along perinephric bridging septa and retroperitoneal interfascial
planes.
A, CT scan at level of mid kidney shows both subcapsular and perinephric hem-
orrhage. Note thickened perinephric bridging septa (arrows).
B, CT scan at level slightly lower than that of A shows perinephric blood decom-
pressing in anterior (open arrow) and posterior (curved arrow) interfascial
planes. Note that descending colon (straight solid arrow) and fat in anterior
pararenal space are uninvolved.
C, CT scan at level of iliac crest shows that blood extending down anterior and
posterior interfascial planes lies in caudal continuation of these structures—the
combined interfascial plane (arrows).
C
AJR:175, August 2000 367
interfascial and lateroconal planes are so inti- diverticulitis, ischemic
Gore et(Fig.
al. 11) and infec- Abdominal Aortic Aneurysm Rupture
mately associated with the retroperitoneal- tious (Fig. 12) colitis, retrocecal appendici- Hemorrhage caused by abdominal aortic
ized ascending and descending mesocolons, tis, and infiltrating colonic neoplasms can aneurysm rupture or disruption of the inferior
the edema and inflammation associated with spread into the interfascial planes. vena cava can communicate with the retro-
Downloaded from www.ajronline.org by 89.130.189.147 on 03/15/18 from IP address 89.130.189.147. Copyright ARRS. For personal use only; all rights reserved
Fig. 8.—Ruptured calyceal fornix with urine decompressing into ante- Fig. 9.—Interfascial dissection of gas. CT scan shows ERCP-related duodenal perforation re-
rior and posterior (curved arrow) interfascial spaces in 60-year-old sulting in dissection of gas in anterior interfascial plane (straight arrow) in 63-year-old man.
woman with obstructive uropathy caused by adenopathy resulting from Scan also shows gas and fluid in posterior interfascial plane (curved arrow).
stage IV cervical cancer. CT scan at level of mid pole of right kidney
shows hydronephrosis and urine dissecting into bridging perinephric
septa. Multiple calcified gallstones are present. Note posterior peri-
nephric (Zuckerkandl’s body) fascia (straight arrow) is separated from
posterior pararenal space by this urinoma.
Fig. 10.—Intraperitoneal and retroperitoneal gas is present on this CT scan of 61-year- Fig. 11.—CT scan of 57-year-old man with schemic colitis shows edema extending into an-
old man with chronic obstructive pulmonary disease, pneumothorax, and retroperito- terior interfascial plane (open arrow), fascial trifurcation (solid arrow), and pericolic fat in
neal and peritoneal extension of air. Note how gas has easily dissected anterior anterior pararenal space. Note marked colonic mural thickening and submucosal edema.
(straight arrow) and posterior (curved arrow) interfascial planes. Intramural dissec-
tion of gas has also occurred in colon.
368 AJR:175, August 2000
Interfascial Decompression Planes of the Retroperitoneum
peritoneum via a number of pathways [26]. present as a groin mass or in the anterior in- the perinephric space that may subsequently in-
Most abdominal aortic aneurysms bleed pos- terfascial plane to cause obstructive jaundice volve the interfascial planes [28].
teriorly and are confined by the psoas space or duodenal or colonic obstruction [27].
or extend into the posterior interfascial plane
Metastatic Disease Summary
behind the left kidney. The inferior vena cava
often bleeds directly into the right posterior Metastatic tumors can spread to the peri- In this perspective, we have presented em-
Downloaded from www.ajronline.org by 89.130.189.147 on 03/15/18 from IP address 89.130.189.147. Copyright ARRS. For personal use only; all rights reserved
interfascial plane [26]. Hemorrhage is often nephric spaces and interfascial planes by several bryologic, anatomic, clinical, and imaging
present in one or both perirenal spaces as mechanisms. Most commonly, paraaortic and evidence that fluid collections originating in
well. The anterior interfascial planes are less pericaval retroperitoneal lymph nodes commu- a retroperitoneal space may exit the space by
commonly involved (Fig. 13). These obser- nicate with small lymph nodes near the renal si- entering easily dissectable planes that result
vations suggest that the abdominal aorta and nus, and these, in turn, connect with small from the embryologic fusion of dorsal me-
inferior vena cava may be continuous with or lymph nodes and a rich network of lymphatics senteries. These planes extend from the dia-
actually reside in the medial aspect of the in the perinephric space [1] (Fig. 14). Pleural phragm to the pelvic floor and appear to be
posterior interfascial plane. and transdiaphragmatic lymphatics communi- an important means by which rapid accumu-
Aortic hemorrhage can also dissect the cate with the superior aspect of the perinephric lating fluid collections and infiltrating dis-
pelvis in the combined interfascial plane and space, providing a pathway of disease spread to eases extend into the retroperitoneum.
Fig. 12.—CT scan of 49-year-old man with pseudomembranous colitis shows mural thick- Fig. 13.—Aortic aneurysm rupture with interfascial spread of retroperitoneal
ening of ascending (AC) and descending (DC) colons. Note inflammation of fat of anterior hematoma (straight arrows) in 73-year-old man. CT scan obtained at level of
pararenal spaces bilaterally. Also note that fluid has extended in anterior (straight arrow) lower pole of left kidney reveals hyperdense hematoma extending across mid-
and posterior (curved arrows) interfascial spaces bilaterally. line in anterior interfascial (retromesenteric) plane bilaterally. On right, he-
matoma also decompresses in posterior interfascial plane (curved arrow).
Fig. 14.—Metastases to perinephric and interfascial spaces from carcinoma of pancreas
in 70-year-old woman. CT scan shows marked retroperitoneal lymphadenopathy (curved
arrow) with tumor spread into anterior interfascial plane (open arrow). Tumor has also in-
filtrated perinephric lymphatics (straight solid arrow).
AJR:175, August 2000 369
Gore et al.
References Philadelphia: Lippincott-Raven, 1998:585–618 Silverman P. Renal fascial pathway: posterior exten-
1. Meyers MA. Dynamic radiology of the abdomen: 10. Dodds WJ, Darweesh RMA, Lawson TL, et al. sion of pancreatic effusions within the anterior parare-
normal and pathologic anatomy, 4th ed. New The retroperitoneal space revisited. AJR 1986; nal space. Radiology 1986;158:367–374
York: Springer, 1994 147:1155–1161 19. Condon RE. Resection of the colon. In: Zuidema
2. Chesbrough RM, Burkhard TK, Martinez AJ, 11. Raptopoulos V, Lei QF, Touliopoulos P, Vrachliotis GA, ed. Schackelford’s surgery of the alimentary
Burks DD. Gerota versus Zuckerkandl: the renal TG, Marks SC Jr. Why perirenal disease does not ex- tract, 4th ed. Philadelphia: Saunders, 1995:207–236
fascia revisited. Radiology 1989;173:845–846 tend into the pelvis: the importance of closure of the 20. Hinman F Jr. Atlas of urological anatomy. Phila-
Downloaded from www.ajronline.org by 89.130.189.147 on 03/15/18 from IP address 89.130.189.147. Copyright ARRS. For personal use only; all rights reserved
3. Aizenstein RI, Wilbur AC, O’Neal HK. Interfas- cone of renal fasciae. AJR 1995;164:1179–1184 delphia: Saunders, 1993:257–268
cial and perinephric pathways in the spread of ret- 12. Kunin M. Bridging septa of the perinephric 21. Yip KTL, Peh WLG, Tam PC. Spontaneous rupture
roperitoneal disease: refined concepts based on space: anatomic, pathologic, and diagnostic con- of renal tumours: the role of imaging in diagnosis
CT observations. AJR 1997;168:639–643 siderations. Radiology 1986;158:361–365 and management. Br J Radiol 1998;71:146–154
4. Aizenstein RI, Owens C, Sabniss S, Wilbur AC, 13. Mindell HJ, Mastromatteo JF, Dickey KW, et al. 22. Kawashima A, Sandler CM, Corriere JN Jr, Rodgers
Hibbeln JF, O’Neil HK. The perinephric space Anatomic communications between the three retro- BM, Goldman SM. Ureteropelvic junction injuries
and renal fascia: review of normal anatomy, pa- peritoneal spaces: determination by CT-guided in- secondary to blunt abdominal trauma. Radiology
thology, and pathways of disease spread. Crit Rev jection of contrast material in cadavers. AJR 1995; 1997;205:487–492
Diagn Imaging 1997;36:325–367 164:1173–1178 23. Lei QF, Marks SC Jr, Touliopoulos P, Raptopou-
5. Molmenti EP, Balfe DM, Kanterman RY, Bennett 14. Kneeland JB, Auh YH, Rubenstein WA, et al. Peri- los V. Fascial planes and compartments of the
HF. Anatomy of the retroperitoneum: observation renal spaces: CT evidence for communication posterior abdomen: the perirenal and pararenal
of the distribution of pathologic fluid collections. along the midline. Radiology 1987;164:657–664 pathways. Clin Anat 1990;3:1–15
Radiology 1996;200:95–103 15. Mastromatteo JF, Mindell HJ, Mastromatteo MF, 24. Korobkin M, Silverman PM, Quint LE, Francis IR.
6. Wagner M, Lawson TL. Segmental anatomy: ap- Magnant MB, Sturtevant NV, Shuman WP. Com- CT of the extraperitoneal space: normal anatomy
plication to clinical medicine. New York: Mac- munications of the pelvic extraperitoneal spaces: and fluid collections. AJR 1992;159:933–941
Millan, 1982 helical CT cadaver study with pelvic extraperito- 25. Rosen A, Korobkin M, Silverman PM, Moor AJ
7. Hureau J, Acossou-Voyeme AK, Germain M, Pradel J. neal injections. Radiology 1997;202:523–530 Jr, Dunnick NR. CT diagnosis of ruptured aortic
Les espaces interpariétonéaux postérieurs ou espaces 16. Beaulieu CF, Mindelzun RE, Dolph J, Jeffrey RB aneurysms. AJR 1984;143:262–268
rétropéritonéaux. I. Anatomia topographique normale. Jr. The infraconal compartment: a multidirec- 26. Parke CE, Stanley RJ, Berlin AJ. Infrarenal vena
Eur J Radiol 1991;72:101–116 tional pathway for the spread of disease between caval injury following blunt trauma: CT findings.
8. Hureau J, Agossou-Voyeme AK, Germain M, Pradel J. the extraperitoneal abdomen and pelvis. J Com- J Comput Assist Tomogr 1993;17:154–157
Les espaces interpariétonéaux postérieurs ou espaces put Assist Tomogr 1997;21:223–228 27. Politoske EJ. Ruptured abdominal aortic aneu-
rétropéritonéaux. II. Anatomia tomodensitomé trique 17. Raptopoulos V, Touliopoulos P, Lei QF, Vrachliotis rysm presenting as an obstruction of the left co-
pathalogique. Eur J Radiol 1991;72:205–227 TG, Marks SC Jr. Medial border of the perirenal lon. Am J Gastroenterol 1990;85:745–747
9. Balfe DM. Normal abdominal and pelvic anatomy. In: space: CT and anatomic correlation. Radiology 28. Wilbur AC, Turk JN, Capek V. Perirenal metastases
Lee JKT, Sagel SS, Stanley RJ, Heiken JP, eds. Com- 1997;205:777–784 from lung cancer: CT diagnosis. J Comput Assist
puted body tomography with MRI correlation, 3rd ed. 18. Raptopoulos V, Kleinman PK, Marks SC Jr, Snyder M, Tomogr 1990;85:745–747
APPENDIX: Terms and Definitions
Interfascial plane: Potential space between layers of renal, lateroconal, or transversalis fascia; result of fusion of embryonic mesentery.
Anterior interfascial retromesenteric plane: Potentially expansile plane between the anterior pararenal and perinephric spaces; continu-
ous across the midline, it is an important potential route of contralateral spread of retroperitoneal collections.
Posterior interfascial retrorenal plane: Potentially expansile plane between the perinephric space and posterior pararenal space; anterior
pararenal, peritoneal, or intrafascial fluid may reside within the retrorenal space.
Lateroconal interfascial plane: Potentially expansile plane between layers of lateroconal fascia; communicates with anterior and posterior
interfascial planes at the fascial trifurcation.
Combined interfascial plane: Potentially expansile plane formed by the inferior blending of the anterior renal, posterior renal, and latero-
conal fasciae; continues into the pelvis, providing a route of disease spread from the abdominal retroperitoneum into the pelvis.
Fascial trifurcation: Site at which the lateroconal fascia emerges from Gerota’s fascia; anterior, posterior, and lateroconal interfascial
planes communicate at the fascial trifurcation, usually located laterally to the kidney.
370 AJR:175, August 2000
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- MCN Review NotesDocument141 pagesMCN Review NotesMelrose Saludares SumugatNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Materiales para Proveedores de Atención MédicaDocument1 pageMateriales para Proveedores de Atención MédicaErnesto Manuel SolisNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Final Draft of Interview TranscriptDocument7 pagesFinal Draft of Interview Transcriptapi-549369201No ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- NAFLD - NASH and Present & Future Management OptionsDocument78 pagesNAFLD - NASH and Present & Future Management OptionsSantosh AnandNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Food Adulteration $ Sbustance AbuseDocument22 pagesFood Adulteration $ Sbustance AbuseBabita Dhruw100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Cluster of Differentiation Antigen PosterDocument1 pageCluster of Differentiation Antigen PosterReeti R. Bhat100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Ag - Ab ReactionsDocument37 pagesAg - Ab ReactionsJennifer DixonNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Organ Dysfunction in SepsisDocument19 pagesOrgan Dysfunction in SepsisRossalia Yuliana100% (1)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Multimorbidity and Its Associated Risk Factors Among Adults in Northern Sudan: A Community-Based Cross-Sectional StudyDocument7 pagesMultimorbidity and Its Associated Risk Factors Among Adults in Northern Sudan: A Community-Based Cross-Sectional StudyOwais SaeedNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Clinical Exercise Pathophysiology For: Physical TherapyDocument595 pagesClinical Exercise Pathophysiology For: Physical TherapyChloe BujuoirNo ratings yet
- 4 5967752355079259055 PDFDocument482 pages4 5967752355079259055 PDFAndre saputra100% (2)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Nursing Care PlanDocument21 pagesNursing Care PlanMeena KoushalNo ratings yet
- JTR - Rabies in Cats Fact Sheet - 06-04-12Document3 pagesJTR - Rabies in Cats Fact Sheet - 06-04-12Lester EvangelistaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- PCE Blueprint 2018 - ENG 1Document11 pagesPCE Blueprint 2018 - ENG 1jamesNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Case Report: Open Fracture 1/3 Distal Os Tibia and Fibula SinistraDocument34 pagesCase Report: Open Fracture 1/3 Distal Os Tibia and Fibula SinistraFarizka Dwinda HNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- National Viral Hepatitis Control Program-Write Up12-07-22Document17 pagesNational Viral Hepatitis Control Program-Write Up12-07-22Harshul SharmaNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- PreeclampsiaDocument9 pagesPreeclampsiaBhawna Sharma67% (3)
- Blood Chem Reference IntervalsDocument3 pagesBlood Chem Reference IntervalsmonnyNo ratings yet
- Chick Lab PresentationDocument12 pagesChick Lab PresentationMarcella (MARCIE) Thanh-GuyetNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- HIV 101 and PharmacologyDocument36 pagesHIV 101 and Pharmacologyjoel contrerasNo ratings yet
- OVJ-2018-04-100 D. GebremichaelDocument9 pagesOVJ-2018-04-100 D. GebremichaelOriosNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Snake BitesDocument21 pagesSnake BitesarifuadNo ratings yet
- World Health Day QuizDocument6 pagesWorld Health Day QuizRenu Syam100% (1)
- SURGERY Breast DiseasesDocument25 pagesSURGERY Breast DiseasesBiplav SinghNo ratings yet
- Asthma, COPD, and Overlap A Case Based Overview of SimilaritiesDocument304 pagesAsthma, COPD, and Overlap A Case Based Overview of SimilaritiesIbrahim SabraNo ratings yet
- Oral Hygiene Toothbrush One Cycle Per SecondDocument3 pagesOral Hygiene Toothbrush One Cycle Per SecondjunquelalaNo ratings yet
- Stanford PulmicortDocument1 pageStanford Pulmicortcbr plansNo ratings yet
- Different Types of Viruses: PoxviridaeDocument6 pagesDifferent Types of Viruses: PoxviridaeMeehsay Senmi MiongNo ratings yet
- Diabetes: Causes, Symptoms and TreatmentsDocument4 pagesDiabetes: Causes, Symptoms and TreatmentsAbdullah BazryNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)