0% found this document useful (1 vote)
2K views1 pageEdpms Service Request Form 2
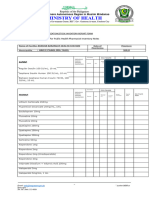
This form requests service from an Electronic Drug Price Monitoring System pharmaceutical division. It collects contact information for the requestor such as name, office, address, phone numbers, and email. It also asks for a description of the request and GPS coordinates. The request must be approved by the head of the requestor's office before being received by pharmaceutical division staff, who then take action and note the request.
Uploaded by
BRENDA BALILICopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (1 vote)
2K views1 pageEdpms Service Request Form 2
This form requests service from an Electronic Drug Price Monitoring System pharmaceutical division. It collects contact information for the requestor such as name, office, address, phone numbers, and email. It also asks for a description of the request and GPS coordinates. The request must be approved by the head of the requestor's office before being received by pharmaceutical division staff, who then take action and note the request.
Uploaded by
BRENDA BALILICopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
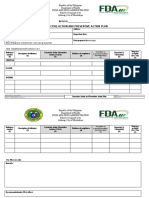
- Service Request Form: This form is used for submitting service requests related to the Electronic Drug Price Monitoring System, collecting essential operational data for address and logistics.