You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Basc-2 Presentation - All SlidesDocument59 pagesBasc-2 Presentation - All Slidesapi-290174387100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
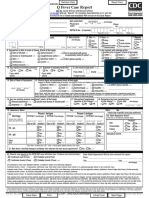
- Q Fever Case Report: Form Approved OMB 0920-0009Document3 pagesQ Fever Case Report: Form Approved OMB 0920-0009Boban ArsovskiNo ratings yet
- AnatomyDocument687 pagesAnatomyBoban ArsovskiNo ratings yet
- TerminologiaAnatomicaafter17years-Inconsistenciesmistakesandnewproposals AA 2015Document10 pagesTerminologiaAnatomicaafter17years-Inconsistenciesmistakesandnewproposals AA 2015Boban ArsovskiNo ratings yet
- Pig Human Comparison PDFDocument15 pagesPig Human Comparison PDFBoban ArsovskiNo ratings yet
- Hypermagnesemia Case PDFDocument2 pagesHypermagnesemia Case PDFBoban ArsovskiNo ratings yet
- Blood TransDocument8 pagesBlood TransWilhelmus Wincent WijayaNo ratings yet
- Hemophilia in ChildrenDocument16 pagesHemophilia in ChildrenVinay Sahu100% (1)
- I Promise MyselfDocument36 pagesI Promise Myselfyodaji60% (5)
- Agricultural Projects, Seminars, Papers, Assignments and EssaysDocument2 pagesAgricultural Projects, Seminars, Papers, Assignments and EssayssoloheaterNo ratings yet
- Nutri-Serve Wellness NewsletterDocument2 pagesNutri-Serve Wellness NewsletterSMSTECHNo ratings yet
- What Are Psychoactive Drugs and How Do They Affect Behavior?Document7 pagesWhat Are Psychoactive Drugs and How Do They Affect Behavior?Roda Gayle RañadaNo ratings yet
- Case Presentation - Closed Fracture Radius Ulna PediatricDocument30 pagesCase Presentation - Closed Fracture Radius Ulna PediatriciamboredtiredNo ratings yet
- Tibetan Buddhist Perspective On HealingDocument12 pagesTibetan Buddhist Perspective On Healingtpspace100% (2)
- Alvarez (1995) - Motiveless Malignity. Problems in The Psychotherapy of Psychopathic PatientsDocument9 pagesAlvarez (1995) - Motiveless Malignity. Problems in The Psychotherapy of Psychopathic PatientsJulián Alberto Muñoz FigueroaNo ratings yet
- Pedo Long AnswerDocument116 pagesPedo Long AnswersamikshaNo ratings yet
- Organic Farming in India: A Vision Towards A Healthy Nation: ReviewDocument8 pagesOrganic Farming in India: A Vision Towards A Healthy Nation: Reviewkatariya vatsalNo ratings yet
- Psicosis - 2021Document30 pagesPsicosis - 2021Felipe VergaraNo ratings yet
- Upper Extremities Parts: Shoulder Girdle Shoulder Joint Elbow Joint Radioulnar Joint Wrist JointDocument30 pagesUpper Extremities Parts: Shoulder Girdle Shoulder Joint Elbow Joint Radioulnar Joint Wrist JointgundadanNo ratings yet
- Animal Circulation and RespirationDocument56 pagesAnimal Circulation and Respirationacooper6No ratings yet
- CASE STUDY #3 Urinary System (Urninary Tract Infection or UTI)Document5 pagesCASE STUDY #3 Urinary System (Urninary Tract Infection or UTI)Lerma PagcaliwanganNo ratings yet
- Kanski Picture TestDocument102 pagesKanski Picture TestAnas Abuseif100% (1)
- Poultry Production and Marketing Project Kitui, KenyaDocument11 pagesPoultry Production and Marketing Project Kitui, KenyaPramod Kumar Chaudhary100% (1)
- HPVDocument3 pagesHPVdsaroha1No ratings yet
- High-Dose Methotrexate With R-CHOP Therapy For The Treatment of Patients With Primary Central Nervous System LymphomaDocument7 pagesHigh-Dose Methotrexate With R-CHOP Therapy For The Treatment of Patients With Primary Central Nervous System LymphomaFariz NurNo ratings yet
- The Therapy of Enzyme Yeast Zell in Cancer. 2001 Serge JurasunasDocument28 pagesThe Therapy of Enzyme Yeast Zell in Cancer. 2001 Serge JurasunaswxcvbnnbvcxwNo ratings yet
- Healing Power of Drumming CirclesDocument2 pagesHealing Power of Drumming CirclesMichael Drake100% (2)
- 6.1 MicrobiologyDocument32 pages6.1 MicrobiologyYsabelle BautistaNo ratings yet
- Aia Flexi PaDocument16 pagesAia Flexi PaNigel LamNo ratings yet
- Diagnostic Accuracy in The Detection of Depth of Myometrial Invasion With MRI in Early-Stage Endometrial CancerDocument5 pagesDiagnostic Accuracy in The Detection of Depth of Myometrial Invasion With MRI in Early-Stage Endometrial CancerBOHR International Journal on GynaecologyNo ratings yet
- Bài Tập Trắc Nghiệm Anh 10- Chương Trình Thí ĐiểmDocument143 pagesBài Tập Trắc Nghiệm Anh 10- Chương Trình Thí ĐiểmPhong ĐâyNo ratings yet
- Angiotensin II Receptor AntagonistDocument1 pageAngiotensin II Receptor AntagonistSonia P SNo ratings yet
- Community PsychologyDocument20 pagesCommunity PsychologyMaePornelaGomezNo ratings yet
- Final Immunisation ApaDocument7 pagesFinal Immunisation ApaLydia ChaiNo ratings yet
- Approach To Jaundice (1) .PPT ALAWAJIDocument28 pagesApproach To Jaundice (1) .PPT ALAWAJIayuNo ratings yet