0% found this document useful (0 votes)
244 views2 pagesTESDA Competency Assessment Form
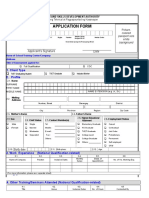
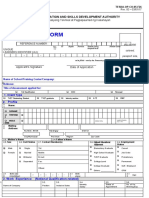
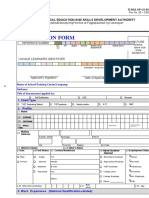
This document is an application form for competency assessment from the Technical Education and Skills Development Authority. It collects information such as the applicant's personal details, educational background, work experience, training attended, licenses and certificates held. The form also includes a section for an admission slip that will be filled out by a processing officer upon acceptance of the application for a specified competency assessment.
Uploaded by
janice ojalesCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOC, PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
244 views2 pagesTESDA Competency Assessment Form
This document is an application form for competency assessment from the Technical Education and Skills Development Authority. It collects information such as the applicant's personal details, educational background, work experience, training attended, licenses and certificates held. The form also includes a section for an admission slip that will be filled out by a processing officer upon acceptance of the application for a specified competency assessment.
Uploaded by
janice ojalesCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOC, PDF, TXT or read online on Scribd