You might also like
- Application FormDocument15 pagesApplication FormHaydeehh BaldinoNo ratings yet
- Application Form OapDocument4 pagesApplication Form OapMike BasalNo ratings yet
- New Application FormsDocument15 pagesNew Application FormsS on the GoNo ratings yet
- Annex 11 - Competency Assessment FormsDocument12 pagesAnnex 11 - Competency Assessment Formsrap leeNo ratings yet
- TESDA APPLICATION FORMDocument2 pagesTESDA APPLICATION FORMmatth bonizaNo ratings yet
- TESDA Application FormDocument3 pagesTESDA Application FormJose MarcoNo ratings yet
- TESDA OP CO 05 Competency Assessment FormsDocument15 pagesTESDA OP CO 05 Competency Assessment FormsDarwin Vargas100% (2)
- TESDA Application FormDocument3 pagesTESDA Application FormRowena Codilla GodoyNo ratings yet
- Evm Ac Form MaranathaDocument2 pagesEvm Ac Form MaranathaEmily De GuzmanNo ratings yet
- APPLICATION-FORM AssessmentDocument2 pagesAPPLICATION-FORM Assessmentkelvsgarcia22No ratings yet
- Application Form New Only 2017Document5 pagesApplication Form New Only 2017Roy AlaNo ratings yet
- Assessment Application Form Long Bond PaperDocument2 pagesAssessment Application Form Long Bond PaperCei mendozaNo ratings yet
- TESDA Application FormDocument3 pagesTESDA Application FormJeg GomezNo ratings yet
- Application Form: Technical Education and Skills Development AuthorityDocument7 pagesApplication Form: Technical Education and Skills Development AuthorityJobert HidalgoNo ratings yet
- TESDA Application FormDocument2 pagesTESDA Application FormMichaelNo ratings yet
- Application Form For AssessmentDocument3 pagesApplication Form For AssessmentIvy Rosell BuayabanNo ratings yet
- TESDA Application FormDocument3 pagesTESDA Application FormMARCELO PELIAS JR.No ratings yet
- TESDA-OP-CO-05 - Competency - Assessment Forms - CSSDocument3 pagesTESDA-OP-CO-05 - Competency - Assessment Forms - CSSMarcNo ratings yet
- Application Form: Technical Education and Skills Development AuthorityDocument3 pagesApplication Form: Technical Education and Skills Development AuthorityMarlon TurturNo ratings yet
- TESDA-OP-CO-05-F26 Application FormDocument3 pagesTESDA-OP-CO-05-F26 Application FormNelianie Bangtuan100% (1)
- Technical Education and Skills Development Authority: Pangasiwaan Sa Edukasyong Teknikal at Pagpapaunlad NG KasanayanDocument3 pagesTechnical Education and Skills Development Authority: Pangasiwaan Sa Edukasyong Teknikal at Pagpapaunlad NG KasanayanAngelica QuisimundoNo ratings yet
- Tesda Application FormDocument1 pageTesda Application FormJACOB OMANGLAD CLARONo ratings yet
- Form TESDADocument2 pagesForm TESDANhor MannNo ratings yet
- Application Forms Competency Assessment FormsDocument2 pagesApplication Forms Competency Assessment FormsAlran Eric Cifra0% (1)
- TESDA Application FormDocument5 pagesTESDA Application FormDaniel SeXan TemporadaNo ratings yet
- TESDA Application FormDocument2 pagesTESDA Application FormOne And All Tech SchoolNo ratings yet
- Application Form (Size A4)Document3 pagesApplication Form (Size A4)Raymart Q. FloresNo ratings yet
- Application-Nc Swiine-IiDocument3 pagesApplication-Nc Swiine-IileonaNo ratings yet
- Application Form BKPDocument3 pagesApplication Form BKPFherlyn FaustinoNo ratings yet
- Application Form: Technical Education and Skills Development AuthorityDocument3 pagesApplication Form: Technical Education and Skills Development AuthorityMark Jay TalisayonNo ratings yet
- Tesda-Op-Co-05 - Tesda Application Form BKP NC Iii 2021Document2 pagesTesda-Op-Co-05 - Tesda Application Form BKP NC Iii 2021KaJong JaclaNo ratings yet
- Application Form: Technical Education and Skills Development AuthorityDocument2 pagesApplication Form: Technical Education and Skills Development AuthorityShekNo ratings yet
- Application Form PharmacyDocument3 pagesApplication Form PharmacyloissyyonlineNo ratings yet
- TESDA Application FormDocument3 pagesTESDA Application FormPete CatindigNo ratings yet
- Assessment Application Forms New TemplateDocument3 pagesAssessment Application Forms New TemplateRue BensonNo ratings yet
- Application-Nc Poultry-IiDocument3 pagesApplication-Nc Poultry-IileonaNo ratings yet
- Application Form: Technical Education and Skills Development AuthorityDocument2 pagesApplication Form: Technical Education and Skills Development AuthorityMary Antoinette FranciscoNo ratings yet
- Application Form-Evm NC IIIDocument2 pagesApplication Form-Evm NC IIIArayaskillsdevt InstitutecorpNo ratings yet
- Application Form: Pangasiwaan Sa Edukasyong Teknikal at Pagpapaunlad NG KasanayanDocument3 pagesApplication Form: Pangasiwaan Sa Edukasyong Teknikal at Pagpapaunlad NG KasanayanJeph Pedrigal0% (1)
- Application Form: Technical Education and Skills Development AuthorityDocument2 pagesApplication Form: Technical Education and Skills Development AuthorityJigs PerezNo ratings yet
- Application Form: Technical Education and Skills Development AuthorityDocument2 pagesApplication Form: Technical Education and Skills Development AuthorityAlran Eric CifraNo ratings yet
- Assessment Application Form 1Document2 pagesAssessment Application Form 1jelly marie floresNo ratings yet
- Application Form: Technical Education and Skills Development AuthorityDocument3 pagesApplication Form: Technical Education and Skills Development AuthorityJeremy OrtegaNo ratings yet
- TESDA Application Forms (6)Document15 pagesTESDA Application Forms (6)HannahNo ratings yet
- TESDACompetency Assessment Application FormsDocument2 pagesTESDACompetency Assessment Application FormsCOBSAT TESDA67% (3)
- Assessment App Form f26 HousekeepingDocument2 pagesAssessment App Form f26 Housekeepingchleo marie dosdosNo ratings yet
- Assessment App Form F26 HousekeepingDocument2 pagesAssessment App Form F26 Housekeepingchleo marie dosdosNo ratings yet
- Application and Self Assessment GuideDocument5 pagesApplication and Self Assessment GuideAnaleen NolascoNo ratings yet
- Application Form: Technical Education and Skills Development AuthorityDocument2 pagesApplication Form: Technical Education and Skills Development AuthorityErnesto OgarioNo ratings yet
- Application Form: Technical Education and Skills Development AuthorityDocument2 pagesApplication Form: Technical Education and Skills Development AuthorityJonathan Cesar Aurellana MendozaNo ratings yet
- APPLICATION FORM NEW For CCA TM1Document2 pagesAPPLICATION FORM NEW For CCA TM1Neil Ian Seth BacaniNo ratings yet
- Application Form: Technical Education and Skills Development AuthorityDocument3 pagesApplication Form: Technical Education and Skills Development AuthorityAbdullah MundasNo ratings yet
- Assessment Center DocumentsDocument10 pagesAssessment Center DocumentsJay MarvinNo ratings yet
- Annex 11 - Competency Assessment Forms - SMAW - ST PEREGRINEDocument3 pagesAnnex 11 - Competency Assessment Forms - SMAW - ST PEREGRINETroyNo ratings yet
- TESDA OP CO 05 Competency Assessment FormsDocument2 pagesTESDA OP CO 05 Competency Assessment FormsVictor M. MorcilloNo ratings yet
- TESDA Application Forms Rev. No. 00-03 - 01 - 17Document2 pagesTESDA Application Forms Rev. No. 00-03 - 01 - 17Karen GraceNo ratings yet
- TESDA-OP-CO-05-F26-Application-Form-2 CGVDocument3 pagesTESDA-OP-CO-05-F26-Application-Form-2 CGVMak mak MacasaetNo ratings yet
- TESDA-OP-CO-05 - Competency - Assessment FormsDocument3 pagesTESDA-OP-CO-05 - Competency - Assessment FormsSweln LayosaNo ratings yet
- English 3 - Quiz # 3 (Week 5-6)Document6 pagesEnglish 3 - Quiz # 3 (Week 5-6)Gilbert Pizarro CabanatanNo ratings yet
- English 3 - Quiz # 1 (Week 1-2)Document6 pagesEnglish 3 - Quiz # 1 (Week 1-2)Gilbert Pizarro CabanatanNo ratings yet
- APECS & Paterson Posture AssessmentDocument8 pagesAPECS & Paterson Posture AssessmentGilbert Pizarro CabanatanNo ratings yet
- English 3 - Quiz # 2 (Week 3-4)Document5 pagesEnglish 3 - Quiz # 2 (Week 3-4)Gilbert Pizarro CabanatanNo ratings yet
- English 3 - Quiz # 3 (Week 7-8)Document6 pagesEnglish 3 - Quiz # 3 (Week 7-8)Gilbert Pizarro CabanatanNo ratings yet
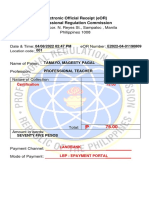
- Electronic Official Receipt (eOR) Professional Regulation CommissionDocument1 pageElectronic Official Receipt (eOR) Professional Regulation CommissionGilbert Pizarro CabanatanNo ratings yet
- Supervise Work Based Learning - Tamayo Magesty FinalDocument41 pagesSupervise Work Based Learning - Tamayo Magesty FinalGilbert Pizarro CabanatanNo ratings yet
- Activity 3 - Invitation To BidDocument2 pagesActivity 3 - Invitation To BidGilbert Pizarro CabanatanNo ratings yet
- Rizal and Philippine History Exam ReviewDocument65 pagesRizal and Philippine History Exam ReviewOda RedNo ratings yet
- GEN ED SET A QuestionairDocument33 pagesGEN ED SET A QuestionairCris Dingayan Jr.No ratings yet
- Session PlanDocument8 pagesSession PlanGilbert Pizarro CabanatanNo ratings yet
- Final Coaching Part 3 Questions and AnswersDocument48 pagesFinal Coaching Part 3 Questions and AnswersR-JayAnteolaNo ratings yet
- APECS & Paterson Posture AssessmentDocument5 pagesAPECS & Paterson Posture AssessmentGilbert Pizarro CabanatanNo ratings yet
- Answer Sheet Name: Magesty P. Tamayo Group: LAOAG Cluster:CLUSTER 1-1Document1 pageAnswer Sheet Name: Magesty P. Tamayo Group: LAOAG Cluster:CLUSTER 1-1Gilbert Pizarro CabanatanNo ratings yet
- Evidence-Plan MagestyDocument1 pageEvidence-Plan MagestyGilbert Pizarro CabanatanNo ratings yet
- GEN ED Mathematics Part 1Document4 pagesGEN ED Mathematics Part 1Danilo Fronda Jr.No ratings yet
- Sample Data Gathering Instrument for Trainee's CharacteristicsDocument19 pagesSample Data Gathering Instrument for Trainee's CharacteristicsGilbert Pizarro CabanatanNo ratings yet
- Sample Data Gathering Instrument For Trainee'S Charactheristics Name of Trainee: Magesty P. Tamayo Characteristics of LearnersDocument11 pagesSample Data Gathering Instrument For Trainee'S Charactheristics Name of Trainee: Magesty P. Tamayo Characteristics of LearnersGilbert Pizarro CabanatanNo ratings yet
- CBLM MagestyDocument43 pagesCBLM MagestyGilbert Pizarro CabanatanNo ratings yet
- Session Plan FinalDocument8 pagesSession Plan FinalGilbert Pizarro CabanatanNo ratings yet
- 3rd Monthly Exam MAPEH 7Document2 pages3rd Monthly Exam MAPEH 7Gilbert Pizarro CabanatanNo ratings yet
- Squat Jump Split Squat Jump Lateral Heiden Depth Jump Single Leg Hop Chest Pass 45 Degree Sit-UpDocument1 pageSquat Jump Split Squat Jump Lateral Heiden Depth Jump Single Leg Hop Chest Pass 45 Degree Sit-UpGilbert Pizarro CabanatanNo ratings yet
- Form 1.1 Self Assessment Check INSTRUCTIONS: This Self-Check Instrument Will Give The Trainer Necessary Data orDocument1 pageForm 1.1 Self Assessment Check INSTRUCTIONS: This Self-Check Instrument Will Give The Trainer Necessary Data orGilbert Pizarro CabanatanNo ratings yet
- Sample data gathering instrument for trainee characteristicsDocument3 pagesSample data gathering instrument for trainee characteristicsGilbert Pizarro CabanatanNo ratings yet
- ACTIVITY 1 - CORE COMPETENCIES-Trainers Methodology 1Document5 pagesACTIVITY 1 - CORE COMPETENCIES-Trainers Methodology 1Gilbert Pizarro Cabanatan100% (1)
- Evidences Proof of Current CompetenciesDocument1 pageEvidences Proof of Current CompetenciesGilbert Pizarro CabanatanNo ratings yet
- Form No 4.4: Training Needs Training Needs (Learning Outcomes) Module Title/Module of InstructionDocument1 pageForm No 4.4: Training Needs Training Needs (Learning Outcomes) Module Title/Module of InstructionGilbert Pizarro CabanatanNo ratings yet
- Identifying Training Gaps-Trainers Methodology 1Document1 pageIdentifying Training Gaps-Trainers Methodology 1Gilbert Pizarro CabanatanNo ratings yet
- Physics: Principles ofDocument20 pagesPhysics: Principles ofNishan SunarNo ratings yet
- Deming 14 Point Almost DoneDocument13 pagesDeming 14 Point Almost DoneAda Ler100% (1)
- A Study of Problems and Prospects of E-Learning in IndiaDocument24 pagesA Study of Problems and Prospects of E-Learning in Indiaarcha agrawalNo ratings yet
- Xii Biomolecules Ncert NotesDocument55 pagesXii Biomolecules Ncert NotesSarita BhattNo ratings yet
- Landscapes of Emotion 1991Document346 pagesLandscapes of Emotion 1991Rachmad AdilaNo ratings yet
- Rizal Lesson 6Document6 pagesRizal Lesson 6Tintin TagupaNo ratings yet
- PMP Exam Prep Training BrochureDocument10 pagesPMP Exam Prep Training BrochureHarendra kumarNo ratings yet
- Detailed Lesson Plan in Science ViDocument6 pagesDetailed Lesson Plan in Science ViJustin Ace MallorcaNo ratings yet
- Best Beginner Guitar Books for KidsDocument3 pagesBest Beginner Guitar Books for Kidstvis MusicNo ratings yet
- Physical Science: Title: Formation of Light Elements in The UniverseDocument26 pagesPhysical Science: Title: Formation of Light Elements in The UniverseLawrence Mae Asong Pamotillo II0% (1)
- Bahasa Inggris (Iklan Pekerjaan)Document5 pagesBahasa Inggris (Iklan Pekerjaan)AndreNo ratings yet
- Preventing child labour study Bhopal marketDocument7 pagesPreventing child labour study Bhopal marketbhobhoNo ratings yet
- Bec Form 137Document2 pagesBec Form 137patrickkayeNo ratings yet
- Data Engineering Study PlanDocument4 pagesData Engineering Study PlanEgodawatta PrasadNo ratings yet
- Zain New CVDocument2 pagesZain New CVZain HaiderNo ratings yet
- Laser Refractive Surgery Privilege RequirementsDocument3 pagesLaser Refractive Surgery Privilege RequirementsYasser BashaNo ratings yet
- 03 Goal-Use Analysis Worksheet-V2.0 (Excel)Document8 pages03 Goal-Use Analysis Worksheet-V2.0 (Excel)Alfredo FloresNo ratings yet
- Ansci95 The Midterm Exam - A NETFLIX Series Article 3Document2 pagesAnsci95 The Midterm Exam - A NETFLIX Series Article 3MARC ANGELO TAMBIADONo ratings yet
- Campus AgresteDocument34 pagesCampus AgresteLetícia SantosNo ratings yet
- 01.21.24 Large Print BulletinDocument10 pages01.21.24 Large Print BulletinFirst Congregational Church of EvanstonNo ratings yet
- 4th Periodical in MAPEH 5Document5 pages4th Periodical in MAPEH 5Airma Ross Hernandez100% (1)
- Critical Analysis Essay PlannerDocument6 pagesCritical Analysis Essay PlannerJersonNo ratings yet
- Rosa ResumeDocument2 pagesRosa Resumeapi-402940629No ratings yet
- 0580 w18 QP 23 PDFDocument12 pages0580 w18 QP 23 PDFHilmar AlfianNo ratings yet
- Download ebook Intermediate Macroeconomics Pdf full chapter pdfDocument67 pagesDownload ebook Intermediate Macroeconomics Pdf full chapter pdfjulia.castro488100% (27)
- Unit 2: Family: I. VocabularyDocument3 pagesUnit 2: Family: I. VocabularyLê VanhNo ratings yet
- Lesson Plan 160205 Jelly Snake PracticalDocument7 pagesLesson Plan 160205 Jelly Snake Practicalapi-309206763No ratings yet
- Pictograms DemonstrationDocument13 pagesPictograms Demonstrationpaula rochaNo ratings yet
- Topic 2 - The Application LetterDocument19 pagesTopic 2 - The Application LetterMad KennyNo ratings yet
- Ethics and Accountability in PhilippineDocument32 pagesEthics and Accountability in PhilippineMelchor Padilla DiosoNo ratings yet