You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Readers PDFDocument155 pagesReaders PDFInfante BRNo ratings yet
- Money Mastermind Vol 1 PDFDocument283 pagesMoney Mastermind Vol 1 PDFKatya SivkovaNo ratings yet
- BS en Iso 06683-2008Document14 pagesBS en Iso 06683-2008bugse100% (1)
- InglesDocument12 pagesInglesInfante BRNo ratings yet
- Installation Italian PDFDocument2 pagesInstallation Italian PDFInfante BRNo ratings yet
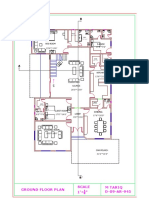
- M Tariq D-09-AR-945 Scale 1' " Ground Floor Plan: 13'6" 9'6" Bed Room S.RoomDocument1 pageM Tariq D-09-AR-945 Scale 1' " Ground Floor Plan: 13'6" 9'6" Bed Room S.RoomInfante BRNo ratings yet
- M Tariq D-09-AR-945 Scale 1' " Ground Floor PlanDocument1 pageM Tariq D-09-AR-945 Scale 1' " Ground Floor PlanInfante BRNo ratings yet
- The Little PriceDocument2 pagesThe Little PriceInfante BRNo ratings yet
- My House PDFDocument1 pageMy House PDFInfante BRNo ratings yet
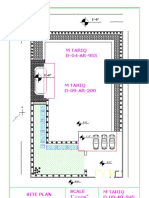
- Pass Plant House PDFDocument1 pagePass Plant House PDFInfante BRNo ratings yet
- The Little PriceDocument2 pagesThe Little PriceInfante BRNo ratings yet
- Pass Plant House PDFDocument1 pagePass Plant House PDFInfante BRNo ratings yet
- Floor plan layout for a residential homeDocument1 pageFloor plan layout for a residential homeInfante BRNo ratings yet
- My NeighborhoodDocument1 pageMy NeighborhoodInfante BRNo ratings yet
- 3 bedroom house floor planDocument1 page3 bedroom house floor planInfante BRNo ratings yet
- TMP 5 A19Document1 pageTMP 5 A19Girraj LakheraNo ratings yet
- Welcome GuideDocument4 pagesWelcome GuideكارينكاجوNo ratings yet
- 1 Man Injured PDFDocument1 page1 Man Injured PDFInfante BRNo ratings yet
- English TranscriptsDocument13 pagesEnglish TranscriptsInfante BRNo ratings yet
- Cats 16052019 PDFDocument1 pageCats 16052019 PDFInfante BRNo ratings yet
- Day of The Dead - MS PDFDocument6 pagesDay of The Dead - MS PDFTung El PulgaNo ratings yet
- Proud PDFDocument18 pagesProud PDFInfante BRNo ratings yet
- Shark in Park Phonics ReaderDocument2 pagesShark in Park Phonics Readerkinayath@yahoo.comNo ratings yet
- SitaDocument27 pagesSitaInfante BRNo ratings yet
- A Christmas CarolDocument45 pagesA Christmas Carolcristina_dumitrescu_1050No ratings yet
- Cards KidsDocument33 pagesCards KidsInfante BR100% (2)
- ls01 PDFDocument4 pagesls01 PDFGustavo SchmidtNo ratings yet
- Thomas T. Scambos, Jr. v. Jack G. Petrie Robert Watson, 83 F.3d 416, 4th Cir. (1996)Document2 pagesThomas T. Scambos, Jr. v. Jack G. Petrie Robert Watson, 83 F.3d 416, 4th Cir. (1996)Scribd Government DocsNo ratings yet
- List Atrazine PDFDocument4 pagesList Atrazine PDFGriffin NuzzoNo ratings yet
- I Love GanzonDocument22 pagesI Love Ganzonarnel tanggaroNo ratings yet
- Biraogo vs. Philippine Truth CommissionDocument3 pagesBiraogo vs. Philippine Truth CommissionJulesMillanarNo ratings yet
- 2020 Dee - v. - Dee Reyes20210424 14 mjb83kDocument4 pages2020 Dee - v. - Dee Reyes20210424 14 mjb83kLynielle CrisologoNo ratings yet
- Chapter06 ProblemsDocument2 pagesChapter06 ProblemsJesús Saracho Aguirre0% (1)
- Sanchez Vs AsinganDocument1 pageSanchez Vs AsinganJanice100% (1)
- Title Pages 1. 2: 22167 Sexuality, Gender and The Law STUDENT ID: 201604269Document21 pagesTitle Pages 1. 2: 22167 Sexuality, Gender and The Law STUDENT ID: 201604269Joey WongNo ratings yet
- Study of Non Performing Assets in Bank of Maharashtra.Document74 pagesStudy of Non Performing Assets in Bank of Maharashtra.Arun Savukar60% (10)
- Types of RoomDocument2 pagesTypes of RoomAran TxaNo ratings yet
- Pi SC4000 17-06 enDocument1 pagePi SC4000 17-06 enAlexandre RogerNo ratings yet
- Instant Download Foundations of Analog and Digital Electronic Circuits Issn PDF FREEDocument32 pagesInstant Download Foundations of Analog and Digital Electronic Circuits Issn PDF FREEjoyce.parkman948100% (43)
- Niva Bupa Health Insurance Company LimitedDocument1 pageNiva Bupa Health Insurance Company LimitedSujanNo ratings yet
- Brasstrax White PaperDocument24 pagesBrasstrax White PaperaramisNo ratings yet
- Joanne Mae VDocument5 pagesJoanne Mae VAndrea Denise VillafuerteNo ratings yet
- Freight RatesDocument16 pagesFreight RatesnishulalwaniNo ratings yet
- Book 1Document9 pagesBook 1Samina HaiderNo ratings yet
- Myths, Heroes and Progress in Mrs. Rania's Speaking ClassDocument26 pagesMyths, Heroes and Progress in Mrs. Rania's Speaking ClassRania ChokorNo ratings yet
- Life of Nelson Mandela, Short Biography of Nelson Mandela, Nelson Mandela Life and Times, Short Article On Nelson Mandela LifeDocument4 pagesLife of Nelson Mandela, Short Biography of Nelson Mandela, Nelson Mandela Life and Times, Short Article On Nelson Mandela LifeAmit KumarNo ratings yet
- Supreme Court Power to Order Change of VenueDocument1 pageSupreme Court Power to Order Change of VenueKathleneGabrielAzasHaoNo ratings yet
- DRS Rev.0 C 051 390 MCC TR2!01!0001 - Condensate StablizationDocument4 pagesDRS Rev.0 C 051 390 MCC TR2!01!0001 - Condensate StablizationBalasubramanianNo ratings yet
- Credit Bureau Development in The PhilippinesDocument18 pagesCredit Bureau Development in The PhilippinesRuben Carlo Asuncion100% (4)
- Election of 2000 WorksheetDocument3 pagesElection of 2000 Worksheetvasanthi sambaNo ratings yet
- Love Is AliveDocument3 pagesLove Is Alivesteven harrisNo ratings yet
- HRDM104 AlmiDocument14 pagesHRDM104 AlmiJessa Joy Alano LopezNo ratings yet
- Case No. 13 - ROBERTO S. BENEDICTO and HECTOR T. RIVERA vs. THE COURT OF APPEALSDocument2 pagesCase No. 13 - ROBERTO S. BENEDICTO and HECTOR T. RIVERA vs. THE COURT OF APPEALSCarmel Grace KiwasNo ratings yet
- Test FAR 570 Feb 2021Document2 pagesTest FAR 570 Feb 2021Putri Naajihah 4GNo ratings yet
- Qualifications approved for direct entry to MRICSDocument7 pagesQualifications approved for direct entry to MRICSJohn BernalteNo ratings yet