You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- BMS1 - K14 - Pharmacotherapy For ParkinsonDocument51 pagesBMS1 - K14 - Pharmacotherapy For ParkinsonAndreNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Burgy PDFDocument6 pagesBurgy PDFAndreNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Infections of The Central Nervous System Radang IDocument120 pagesInfections of The Central Nervous System Radang IAndreNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- BMS1 - K4 - K5 - K6 - Electrical Activity of The Brain, Sleep-Wake States, and Circadian RythmsDocument72 pagesBMS1 - K4 - K5 - K6 - Electrical Activity of The Brain, Sleep-Wake States, and Circadian RythmsAndreNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- BMS1 - K11 - Pathology of Peripheral Nerve and Central Nervous SystemDocument60 pagesBMS1 - K11 - Pathology of Peripheral Nerve and Central Nervous SystemAndreNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Computed Tomography (CT) in Blunt Liver Injury: A Pictorial EssayDocument7 pagesComputed Tomography (CT) in Blunt Liver Injury: A Pictorial EssayAndreNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Terapi SCC Kemo RadiasiDocument42 pagesTerapi SCC Kemo RadiasiAndreNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- (20834594 - Anthropological Review) Relationship Between Type and Weight of Placenta and Neonate Birth Weight in Twin PregnancyDocument10 pages(20834594 - Anthropological Review) Relationship Between Type and Weight of Placenta and Neonate Birth Weight in Twin PregnancyAndreNo ratings yet
- By: Andre Patarsaroha S (120100201) Khawjiaqian (120100451) Supervisor: Dr. Dr. Okerinaramayani, SP A (K)Document38 pagesBy: Andre Patarsaroha S (120100201) Khawjiaqian (120100451) Supervisor: Dr. Dr. Okerinaramayani, SP A (K)AndreNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Stroke Acute StrokeDocument16 pagesStroke Acute StrokeAndreNo ratings yet
- Gds 138 Slide Childhood ObesityDocument11 pagesGds 138 Slide Childhood ObesityAndreNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- (09032021) Press Release For Resumption of Selected Sports For NSG 2021 - MOEDocument2 pages(09032021) Press Release For Resumption of Selected Sports For NSG 2021 - MOEthesuperprogamer2 gamerNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- WWW - England.nhs - Uk: Business Continuity Management NHS WorkshopDocument52 pagesWWW - England.nhs - Uk: Business Continuity Management NHS WorkshopForbetNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Medic Shoes - Clinic Report - 25/10/2020Document49 pagesMedic Shoes - Clinic Report - 25/10/2020יפה גולןNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Cox, D.R. - Donnelly, C.A. - Principles of Applied StatisticsDocument209 pagesCox, D.R. - Donnelly, C.A. - Principles of Applied Statisticstgabi2012No ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Complementary and Alternative Health Care Client Bill of RightsDocument2 pagesComplementary and Alternative Health Care Client Bill of Rightsapi-31121402No ratings yet
- Neonatal Antiepileptic Medication Treatment Patterns A Decade of ChangeDocument8 pagesNeonatal Antiepileptic Medication Treatment Patterns A Decade of ChangeEduardo Rios DuboisNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- LifebuoyDocument10 pagesLifebuoyPrateek Gupta100% (1)
- Correcta Posicion Del TornilloDocument5 pagesCorrecta Posicion Del TornilloSilvia PluisNo ratings yet
- PANCE Word Associations PDFDocument27 pagesPANCE Word Associations PDFkatNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- DR Axe 5 Essential Oils Proven Bymedical Science PDFDocument7 pagesDR Axe 5 Essential Oils Proven Bymedical Science PDFDubravka Duda100% (1)
- Coxa PlanaDocument9 pagesCoxa PlanaRegine BlanzaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- RAGHU Final ProjectDocument50 pagesRAGHU Final ProjectPrakashNo ratings yet
- RBI Grade B - 2021 - Phase - 1 - EveningDocument54 pagesRBI Grade B - 2021 - Phase - 1 - EveningPRIYANSHU LAWANIANo ratings yet
- Letter To ParentsDocument4 pagesLetter To ParentsGary DetmanNo ratings yet
- Pubmed - Australia - Clinical - brokenAffLastHistoDocument131 pagesPubmed - Australia - Clinical - brokenAffLastHistoHNNo ratings yet
- Donut Hole LetterDocument2 pagesDonut Hole LetterPeter SullivanNo ratings yet
- Symbicort Rapihaler (Budesonide and Formoterol Fumarate Dihydrate) Drug MediciDocument14 pagesSymbicort Rapihaler (Budesonide and Formoterol Fumarate Dihydrate) Drug Medicijr7mondo7edoNo ratings yet
- Anti Smoking Laua-AnDocument2 pagesAnti Smoking Laua-AnraemmmanlagradaNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
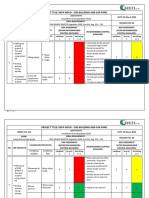
- 013 HIRARC Installation of Hoisting BeamDocument8 pages013 HIRARC Installation of Hoisting Beambdiey100% (1)
- 51 Ijmrp 3 (6) 263-65Document3 pages51 Ijmrp 3 (6) 263-65ahmed samirNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- E & MDocument8 pagesE & MAnonymous MtKJkerbpU75% (4)
- Jerusalem SyndromeDocument5 pagesJerusalem Syndromele_papillon15No ratings yet
- Labor 1 CruzDocument9 pagesLabor 1 CruzKym AlgarmeNo ratings yet
- Literature Review On OgiDocument7 pagesLiterature Review On Ogiafdtaeczo100% (1)
- 1.neuro Intro-1 UMTDocument51 pages1.neuro Intro-1 UMTLOVELY WALEEDNo ratings yet
- LSDE July 30 Tuesday 2013Document8 pagesLSDE July 30 Tuesday 2013LeyteSamar DailyExpressNo ratings yet
- Psychopharma 1Document7 pagesPsychopharma 1Mitchee Zialcita100% (1)
- CHOLElithiasisDocument93 pagesCHOLElithiasisfranciscomaricris13No ratings yet
- Ansi A10.42Document23 pagesAnsi A10.42pedro la rosa100% (1)
- UCD School of Medicine Undergraduate Prospectus 2022-1Document36 pagesUCD School of Medicine Undergraduate Prospectus 2022-1ARab COMPutersNo ratings yet