You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- ENT 1.2 Diseases of The Nose, Paranasal Sinuses, and Face PDFDocument18 pagesENT 1.2 Diseases of The Nose, Paranasal Sinuses, and Face PDFZazaNo ratings yet
- Invisible Minerals Part I Magnesium: DisclaimerDocument119 pagesInvisible Minerals Part I Magnesium: DisclaimerhemanthalNo ratings yet
- Homeopathic Remedies For 'Flu - Flow ChartDocument1 pageHomeopathic Remedies For 'Flu - Flow Chartisadore97% (31)
- Diastolic DysfunctionDocument30 pagesDiastolic DysfunctionMateo Uribe MorenoNo ratings yet
- PREFACE: " Chronic Fatigue Syndrome: A Guide To The Homeopathic Treatment of CFS/M.E."Document5 pagesPREFACE: " Chronic Fatigue Syndrome: A Guide To The Homeopathic Treatment of CFS/M.E."Diane SolomonNo ratings yet
- Odontogenic and Non Odontogenic PainDocument100 pagesOdontogenic and Non Odontogenic Painsanket pandeyNo ratings yet
- Lotus Theory and DiseaseDocument4 pagesLotus Theory and DiseaseG AnshuNo ratings yet
- ECG Interpretation Made Incredibly Easy! (5th Edition)Document6 pagesECG Interpretation Made Incredibly Easy! (5th Edition)Islam AminNo ratings yet
- Where There Is No PsychiatristDocument335 pagesWhere There Is No PsychiatristIFANI NURUL ISLAMYNo ratings yet
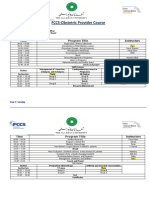
- FCCS-Obstetric Provider Course: Time Program Title InstructorsDocument2 pagesFCCS-Obstetric Provider Course: Time Program Title InstructorsSamina AyazNo ratings yet
- What Protections Does The Upper Airway Have For The Lower Airway?Document3 pagesWhat Protections Does The Upper Airway Have For The Lower Airway?Paul JacksonNo ratings yet
- Postural Drainage in EnglishDocument3 pagesPostural Drainage in EnglishIndra SajhaNo ratings yet
- Bahasa Inggris SOALDocument20 pagesBahasa Inggris SOALAyu Nita PangestuNo ratings yet
- Acute Exacerbation of AsthmaDocument33 pagesAcute Exacerbation of Asthmafrankozed1No ratings yet
- Aloe Vera As SoapDocument5 pagesAloe Vera As SoapAxel Klise100% (1)
- SCD Factsheet What Is SCDDocument5 pagesSCD Factsheet What Is SCDAustine OsaweNo ratings yet
- Of' The: BishopDocument11 pagesOf' The: BishopAnnisa FebriezaNo ratings yet
- Exalted 3ed Core - Rules - Removed Parts v1Document20 pagesExalted 3ed Core - Rules - Removed Parts v1Rafael SoaresNo ratings yet
- Saint Lucia-Blank Maritime Declaration of HealthDocument3 pagesSaint Lucia-Blank Maritime Declaration of HealthjruitNo ratings yet
- Defining Autism (Martha Herbert, M.D.)Document52 pagesDefining Autism (Martha Herbert, M.D.)National Press FoundationNo ratings yet
- Why Students Should Eat Breakfast EverydayDocument8 pagesWhy Students Should Eat Breakfast EverydayEarly Vici Azmia0% (1)
- Centenary Ch4Document12 pagesCentenary Ch4ferisiswonoNo ratings yet
- Medical Terms in Lay Language2Document7 pagesMedical Terms in Lay Language2Mavra zNo ratings yet
- PS 5 Lec 1 IntroDocument9 pagesPS 5 Lec 1 IntronickalecdecesareNo ratings yet
- Stroke Reports Following Covid VaccineDocument9 pagesStroke Reports Following Covid VaccineJosh Singer100% (2)
- Second Hand SmokerDocument7 pagesSecond Hand SmokerNafisNo ratings yet
- Prepared By: Manisha Thapa Leeza ShresthaDocument12 pagesPrepared By: Manisha Thapa Leeza ShresthaManjesh Mishra XettriNo ratings yet
- Senior Care Plan (: For Ages 61-100 Yrs Old)Document7 pagesSenior Care Plan (: For Ages 61-100 Yrs Old)Clarissa RefugioNo ratings yet
- Whipple ProcedureDocument8 pagesWhipple ProcedureDae AhmadNo ratings yet
- Mariko Aoki PhenomenonDocument19 pagesMariko Aoki PhenomenonChristopher ServantNo ratings yet