You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (843)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Student Teaching Reflective Essay RevisedDocument35 pagesStudent Teaching Reflective Essay Revisedapi-439274163100% (1)
- Point S Aralia Racem OSADocument7 pagesPoint S Aralia Racem OSArahimnoorNo ratings yet
- DS160 Service Manual English 1Document64 pagesDS160 Service Manual English 1Roman Cupul RuizNo ratings yet
- Bacteriological Examination of Drinking Water (English Edition)Document68 pagesBacteriological Examination of Drinking Water (English Edition)Abdurazzaq Altomi93% (15)
- Latinhymnswithen00marcuoft PDFDocument358 pagesLatinhymnswithen00marcuoft PDFDavid DávilaNo ratings yet
- Topological Insulators and Superconductors Lecture PDFDocument19 pagesTopological Insulators and Superconductors Lecture PDFbphysicssNo ratings yet
- Diagnostic Test English 4Document4 pagesDiagnostic Test English 4Christine Marie OraizNo ratings yet
- Exercises - Many. Much, A Lot of .Doc - StudentDocument7 pagesExercises - Many. Much, A Lot of .Doc - StudentFrancisco OliveiraNo ratings yet
- Tugade Vs Court of AppealsDocument3 pagesTugade Vs Court of AppealsAngelo GabrilloNo ratings yet
- Running Head: Harvard Business Case Study: Infosys Group 1Document5 pagesRunning Head: Harvard Business Case Study: Infosys Group 1Anonymous RoAnGpANo ratings yet
- Mabini CollegesDocument4 pagesMabini CollegesRobert Ross DulayNo ratings yet
- IST Practice Test 15 16Document9 pagesIST Practice Test 15 16Maria CindaNo ratings yet
- Tunnelling Under Squeezing ConditionsDocument30 pagesTunnelling Under Squeezing ConditionsCarmine TranfaNo ratings yet
- Chap 02 (Fluid Mechanic) PDFDocument65 pagesChap 02 (Fluid Mechanic) PDFK'roll Azham AvearNo ratings yet
- Evaluation of The Spitzkasten Classifier in Terms of Hydraulic Velocity and Mass RecoveryDocument41 pagesEvaluation of The Spitzkasten Classifier in Terms of Hydraulic Velocity and Mass RecoveryAllen DimayugaNo ratings yet
- Transcendental Idealism of GermanyDocument11 pagesTranscendental Idealism of GermanyAshleshaMittalNo ratings yet
- (Worlds of Desire - The Chicago Series On Sexuality, Gender, and Culture) Stephen O. Murray - Homosexualities - University of Chicago Press (2000) PDFDocument261 pages(Worlds of Desire - The Chicago Series On Sexuality, Gender, and Culture) Stephen O. Murray - Homosexualities - University of Chicago Press (2000) PDFanon_937785226100% (1)
- Osteomyelitis: Dr. Sunil Pahari 2 Year Resident Department of Orthopedics Yangtze UniversityDocument48 pagesOsteomyelitis: Dr. Sunil Pahari 2 Year Resident Department of Orthopedics Yangtze UniversityPercy Linares MorilloNo ratings yet
- David Walliams Writing Childrens Books V1Document64 pagesDavid Walliams Writing Childrens Books V1Tatjana KeninaNo ratings yet
- Quali Vs QuantiDocument4 pagesQuali Vs QuantiMGPagaduanNo ratings yet
- SPE 113995 Investigation of Diffusion Coefficients of Heavy Oil and Hydrocarbon Solvent Systems in Porous MediaDocument10 pagesSPE 113995 Investigation of Diffusion Coefficients of Heavy Oil and Hydrocarbon Solvent Systems in Porous MediaJair NaranjoNo ratings yet
- 3204 s04 QP 2Document8 pages3204 s04 QP 2Souradeep SahaNo ratings yet
- Grade 5 Daily Lesson Log: Joel F. GautDocument4 pagesGrade 5 Daily Lesson Log: Joel F. GautJoel GautNo ratings yet
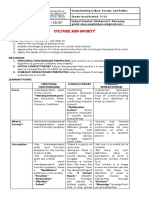
- Culture and Society: Module 2 - UcspDocument3 pagesCulture and Society: Module 2 - Ucspkimberson alacyangNo ratings yet
- McDonalds Case StudyDocument2 pagesMcDonalds Case Studyshax001No ratings yet
- Physics Lab ManualDocument62 pagesPhysics Lab ManualKrishna MahajanNo ratings yet
- Special Issue "Stability and Nonlinear Analysis of Steel Structures - Research Advances"Document228 pagesSpecial Issue "Stability and Nonlinear Analysis of Steel Structures - Research Advances"biomechanicsNo ratings yet
- People v. Bonifacio y SiaoDocument7 pagesPeople v. Bonifacio y SiaosdysangcoNo ratings yet
- More Punnett PracticeDocument2 pagesMore Punnett Practiceking bossNo ratings yet
- Course Outcomes COs For All Programmes - 2021 22 Reference MiteDocument108 pagesCourse Outcomes COs For All Programmes - 2021 22 Reference MiteNischitha PNo ratings yet