You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Nursing Care Plan Ineffective Airway ClearanceDocument3 pagesNursing Care Plan Ineffective Airway Clearancederic100% (13)
- Menopause Health QuestionnaireDocument8 pagesMenopause Health QuestionnaireFatma Risda HidayantiNo ratings yet
- Off Label Drug - Bu SintaDocument18 pagesOff Label Drug - Bu SintaChandra NiansariNo ratings yet
- Establish A Pulmonary Rehabilitation Programme: Done By: Amina Issa Sarah Yaqoob Norhan Howary Shahad Al - HammadDocument18 pagesEstablish A Pulmonary Rehabilitation Programme: Done By: Amina Issa Sarah Yaqoob Norhan Howary Shahad Al - HammadAmina SawalmehNo ratings yet
- Jahshan OET Collection E2L LISTENING T1 EDocument8 pagesJahshan OET Collection E2L LISTENING T1 EP.K.No ratings yet
- 40th Anniversary BookletUHMSDocument59 pages40th Anniversary BookletUHMSmiguek clementsNo ratings yet
- Mountain Province Vaccination Monitoring: Data (As of October 24-30, 2021)Document14 pagesMountain Province Vaccination Monitoring: Data (As of October 24-30, 2021)Janice DinesNo ratings yet
- Bon Secours Resume Post-Grad PortfolioDocument2 pagesBon Secours Resume Post-Grad Portfolioapi-578141969No ratings yet
- Drug Proving Is The Systematic Process of Acquiring Knowledge of The Instruments Intended For The Cure ofDocument4 pagesDrug Proving Is The Systematic Process of Acquiring Knowledge of The Instruments Intended For The Cure ofKamal PatidarNo ratings yet
- Formularium Nasional: Analgetik Non NarkotikDocument2 pagesFormularium Nasional: Analgetik Non Narkotikyauminnisa hapsariNo ratings yet
- DAFTAR PUSTAKAeeDocument3 pagesDAFTAR PUSTAKAeenidhya05No ratings yet
- Pharmacokinetics: Dr. Mizanur RahmanDocument46 pagesPharmacokinetics: Dr. Mizanur Rahmangl tousifNo ratings yet
- Medication Errors: P AperDocument4 pagesMedication Errors: P Aperdesk ayu okaNo ratings yet
- Reimbursement ProformaDocument6 pagesReimbursement ProformaMahesh DewaniNo ratings yet
- TesticularDocument79 pagesTesticularAndryanto リクア SutantoNo ratings yet
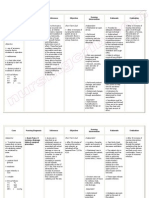
- Name Classification Action Indication Adverse Effect Contraindication Nursing ConsiderationDocument3 pagesName Classification Action Indication Adverse Effect Contraindication Nursing ConsiderationSonny Dizon PareñasNo ratings yet
- Allen College of Homoeopathy: LycopodiumDocument4 pagesAllen College of Homoeopathy: Lycopodiumtriptee100% (1)
- Pain Control With Acupuncture - Class 2Document46 pagesPain Control With Acupuncture - Class 2Hector Rojas100% (2)
- 3.evaluation and Examination of Dental PatientsDocument77 pages3.evaluation and Examination of Dental PatientscreativejoburgNo ratings yet
- Orthopedics Notes NeetpgDocument4 pagesOrthopedics Notes NeetpgGIST (Gujarat Institute of Science & Technology)No ratings yet
- Dr. Smith's ECG Blog - "Shark Fin" - A Deadly ECG Sign That You Must Know! PDFDocument7 pagesDr. Smith's ECG Blog - "Shark Fin" - A Deadly ECG Sign That You Must Know! PDFZACHARIAH MANKIRNo ratings yet
- Simposium Iii. 2. Guch. Dr. L. Krisdinarti SPPD SPJPK PDFDocument33 pagesSimposium Iii. 2. Guch. Dr. L. Krisdinarti SPPD SPJPK PDFbagus krisnaNo ratings yet
- AntimicrobialDocument211 pagesAntimicrobialSanaz Niksefat100% (1)
- (CPG) Update of The Clinical Practice Guidelines On The Diagnosis and Management of Nicotine Dependence 2021Document90 pages(CPG) Update of The Clinical Practice Guidelines On The Diagnosis and Management of Nicotine Dependence 2021Jereel Hope Bacon100% (1)
- DR Vernon Coleman The PCR Test Can Kill You - and Can Be Used To Vaccinate YouDocument3 pagesDR Vernon Coleman The PCR Test Can Kill You - and Can Be Used To Vaccinate YouGeorge Kouris100% (1)
- BR 202252Document1 pageBR 202252Indiana Family to FamilyNo ratings yet
- Daftar Pustaka FixDocument3 pagesDaftar Pustaka FixRotua Uli CarolinaNo ratings yet
- Inspection Observations FY19 0Document410 pagesInspection Observations FY19 0anissa amalliaNo ratings yet
- Normocytic AnemiaDocument16 pagesNormocytic AnemiaPaula ArayaNo ratings yet
- Follow Ryans Healing Adventure With Stage 4 CancerDocument2 pagesFollow Ryans Healing Adventure With Stage 4 CancerMNo ratings yet