You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Diare 3Document5 pagesDiare 3faizah sugiartoNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- ZoomraokeDocument3 pagesZoomraokefaizah sugiartoNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Motiv Letter Sebelum RevisiDocument5 pagesMotiv Letter Sebelum Revisifaizah sugiartoNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Diare 3Document5 pagesDiare 3faizah sugiartoNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- DiareeeeeDocument10 pagesDiareeeeefaizah sugiartoNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Scientific Paper Appraisal: Conclusion: Complete/Not CompleteDocument2 pagesScientific Paper Appraisal: Conclusion: Complete/Not Completefaizah sugiartoNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- 177Document3 pages177faizah sugiartoNo ratings yet
- English Belum EditDocument5 pagesEnglish Belum Editfaizah sugiartoNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- English Belum EditDocument5 pagesEnglish Belum Editfaizah sugiartoNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hist OOOOODocument13 pagesHist OOOOOfaizah sugiartoNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
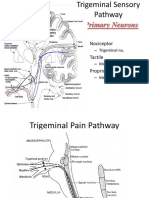
- Primary Neurons: - Nociceptor - Tactile - ProprioceptiveDocument7 pagesPrimary Neurons: - Nociceptor - Tactile - Proprioceptivefaizah sugiartoNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Identifikasi Candida Albicans Dengan Germ TubeDocument2 pagesIdentifikasi Candida Albicans Dengan Germ Tubefaizah sugiartoNo ratings yet
- EnamelDocument1 pageEnamelfaizah sugiartoNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Linguistic Units and Speech Production Theory: Citation: View Online: View Table of Contents: Published by TheDocument3 pagesLinguistic Units and Speech Production Theory: Citation: View Online: View Table of Contents: Published by Thefaizah sugiartoNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Approach, Mosby, St. LouisDocument1 pageApproach, Mosby, St. Louisfaizah sugiartoNo ratings yet
- Hubungan Kebiasaan Merokok Dengan Penyakit Periodontal Karyawanpt. Family Raya Gurun Laweh Lubuk Begalung PadangDocument4 pagesHubungan Kebiasaan Merokok Dengan Penyakit Periodontal Karyawanpt. Family Raya Gurun Laweh Lubuk Begalung Padangfaizah sugiartoNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Perbedaan MorfologiDocument5 pagesPerbedaan Morfologifaizah sugiartoNo ratings yet
- Embriogenesis: Faizah Sugiarto - Himawan ArgoDocument18 pagesEmbriogenesis: Faizah Sugiarto - Himawan Argofaizah sugiartoNo ratings yet
- Structure EnamelDocument4 pagesStructure Enamelfaizah sugiartoNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Structure EnamelDocument4 pagesStructure Enamelfaizah sugiartoNo ratings yet
- Cover Laporan Tutorial HumanioraDocument2 pagesCover Laporan Tutorial Humaniorafaizah sugiartoNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- AIQ First Round Allotment 2020 PDFDocument403 pagesAIQ First Round Allotment 2020 PDFVenkatram AnnamdevaraNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- HRNBL1-ESIOP Protocol Anglais Amendement4 Juillet2009Document303 pagesHRNBL1-ESIOP Protocol Anglais Amendement4 Juillet2009Bianca Alexandra100% (1)
- PANCE Word AssociationDocument27 pagesPANCE Word Associationlevmette100% (8)
- 2.1 Kebijakan Pengendalian Kanker Indonesia (DR Ina)Document25 pages2.1 Kebijakan Pengendalian Kanker Indonesia (DR Ina)Agung NugrohoNo ratings yet
- Anatomy of The Endocrine SystemDocument9 pagesAnatomy of The Endocrine SystemMesum Jutt100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Via Module NicprDocument16 pagesVia Module Nicprpedjoang fkupr2017No ratings yet
- Nefropatia Mesoamericana Tablas e ImagenesDocument16 pagesNefropatia Mesoamericana Tablas e ImagenesRosanaDíazNo ratings yet
- Air Pollution's Link to AsthmaDocument15 pagesAir Pollution's Link to AsthmaRavi KantNo ratings yet
- Chromate Primer Paints: HSE Information SheetDocument4 pagesChromate Primer Paints: HSE Information SheetJorge Arana YiNo ratings yet
- BibliographyDocument21 pagesBibliographyapi-204960846No ratings yet
- Punjab An Environmental Health Hotspot Heading Towards DeathDocument12 pagesPunjab An Environmental Health Hotspot Heading Towards DeathDr. Amar Singh AzadNo ratings yet
- Exercise in PregnancyDocument7 pagesExercise in PregnancynirchennNo ratings yet
- General Physical Examination: IAP UG Teaching Slides 2015-16Document49 pagesGeneral Physical Examination: IAP UG Teaching Slides 2015-16Zahra PainterNo ratings yet
- Oral Medicine FinalDocument29 pagesOral Medicine Finallenami_91No ratings yet
- SPINAL CORD INJURY OVERVIEWDocument59 pagesSPINAL CORD INJURY OVERVIEWfazliahNo ratings yet
- Literature Review on the Impact of HIV/AIDSDocument148 pagesLiterature Review on the Impact of HIV/AIDSstelandreouNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Chronic Fatigue Syndrome Caused by Electromagnetic Fields (EMF) ?Document6 pagesChronic Fatigue Syndrome Caused by Electromagnetic Fields (EMF) ?SwissTeslaNo ratings yet
- Goodheart's Photoguide of Common Skin Disorders, 3E (2009) (PDF) (UnitedVRG)Document696 pagesGoodheart's Photoguide of Common Skin Disorders, 3E (2009) (PDF) (UnitedVRG)Alina Banica100% (7)
- Liver: Southern Technical University Collage of Health and Medical Technology Department of Medical Lab TechnologyDocument6 pagesLiver: Southern Technical University Collage of Health and Medical Technology Department of Medical Lab Technologymortda jassimNo ratings yet
- Disorders of Adrenal GlandsDocument48 pagesDisorders of Adrenal GlandsCharlz ZipaganNo ratings yet
- Paroxysmal Nocturnal Hemoglobinuria Testing in Patients With Myelodysplastic Syndrome in Clinical PracticeDocument7 pagesParoxysmal Nocturnal Hemoglobinuria Testing in Patients With Myelodysplastic Syndrome in Clinical PracticeNancy Fanny Vega ZuñigaNo ratings yet
- SchistosomiasisDocument3 pagesSchistosomiasisJohanna Mae DNonoNo ratings yet
- Earnose 1 10091Document4 pagesEarnose 1 10091Annisa KartikasariNo ratings yet
- Cancer Is A Fungus ... and It Is Curable - David Icke WebsiteDocument9 pagesCancer Is A Fungus ... and It Is Curable - David Icke WebsiteIvan100% (2)
- Clinical Biochemistry ReviewDocument10 pagesClinical Biochemistry Reviewyaykatai100% (2)
- Endocrine System (Pathophysiology)Document18 pagesEndocrine System (Pathophysiology)roselle legson100% (1)
- History (Awasir)Document37 pagesHistory (Awasir)Yousef TaqatqehNo ratings yet
- HSC 394 Final ProjectDocument57 pagesHSC 394 Final Projectapi-285024562No ratings yet
- Essential Fatty Acids: What Makes Them Essential and BeneficialDocument3 pagesEssential Fatty Acids: What Makes Them Essential and BeneficialMa.Ysabelle TaclaNo ratings yet
- Organ Sale and DonationDocument61 pagesOrgan Sale and DonationSachin PatelNo ratings yet