You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5808)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (843)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Medical Gas Piping SpecDocument22 pagesMedical Gas Piping Specvvg100% (1)
- 3902 Engl 2012 111 PDFDocument67 pages3902 Engl 2012 111 PDFvcock6109No ratings yet
- ITF Bulls Eye BatchDocument4 pagesITF Bulls Eye BatchDecoded 1 Mr unknownNo ratings yet
- Design of Composite Columns: The American Approach: Roberto T. LeonDocument18 pagesDesign of Composite Columns: The American Approach: Roberto T. LeonvardhangargNo ratings yet
- HZ Rac Tor Tun Unn Lla Tor: 10 G Va Edg OsciDocument4 pagesHZ Rac Tor Tun Unn Lla Tor: 10 G Va Edg OsciΑΝΔΡΕΑΣ ΤΣΑΓΚΟΣNo ratings yet
- Irrigationchannelsnxpowerlite 150327075134 Conversion Gate01Document88 pagesIrrigationchannelsnxpowerlite 150327075134 Conversion Gate01Muhammad UsmanNo ratings yet
- Nexgen Complete Knee Solution Epicondylar Instrumentation Surgical Technique For Legacy Posterior Stabalized Knees Surgical TechniqueDocument32 pagesNexgen Complete Knee Solution Epicondylar Instrumentation Surgical Technique For Legacy Posterior Stabalized Knees Surgical TechniqueTudor MadalinaNo ratings yet
- ACM Problem Set Volume 1Document169 pagesACM Problem Set Volume 1蘇意喬No ratings yet
- Lupus NephritisDocument39 pagesLupus NephritisGowrisangarNo ratings yet
- The Polysphere BOOK #ONEDocument63 pagesThe Polysphere BOOK #ONECGBENJNo ratings yet
- Mcqs Mth301 SolvedDocument24 pagesMcqs Mth301 Solvedcs619finalproject.com92% (12)
- AIRBUS Brochure CompressedDocument54 pagesAIRBUS Brochure CompressedEmmanuel Rei ZamoraNo ratings yet
- Peri-Urbanization - Zones of Rural-Urban TransitionDocument10 pagesPeri-Urbanization - Zones of Rural-Urban TransitionVijay Krsna100% (1)
- R H ParmarDocument7 pagesR H ParmarSumit ParmarNo ratings yet
- Astm g21 g22Document7 pagesAstm g21 g22ENZO CORSI0% (1)
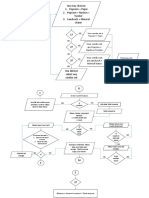
- FlowchartDocument3 pagesFlowchartSarah SazaliNo ratings yet
- CP 150 Specifications SheetDocument2 pagesCP 150 Specifications SheetSergio D. Mercado VeraNo ratings yet
- Electronegativity QuestionsDocument3 pagesElectronegativity QuestionsThe ImmortalNo ratings yet
- JMC 04, Block 2 1523967659Document74 pagesJMC 04, Block 2 1523967659Surabhi TiwariNo ratings yet
- Dubai Stopovers: Hotel Reference GuideDocument2 pagesDubai Stopovers: Hotel Reference Guiderupinder_gujral5102No ratings yet
- Dewey (1896) The Reflex Arc Concept in PsychologyDocument14 pagesDewey (1896) The Reflex Arc Concept in PsychologyLeonardo GomesNo ratings yet
- MSDS - White GlueDocument10 pagesMSDS - White Gluedoan leNo ratings yet
- Volvo ConstrutionDocument59 pagesVolvo ConstrutionCarlosNo ratings yet
- The RenaissanceDocument2 pagesThe RenaissanceTeresa ValverdeNo ratings yet
- Rising Action Exposition: MoanaDocument2 pagesRising Action Exposition: MoanaElyn SabordoNo ratings yet
- Anthropology AssignemnetDocument20 pagesAnthropology AssignemnetabiyNo ratings yet
- Hull & Machinery Survey Report - MV FRI SKY - Damage To Auxiliary Engine Ref. 471-S-2020 PDFDocument43 pagesHull & Machinery Survey Report - MV FRI SKY - Damage To Auxiliary Engine Ref. 471-S-2020 PDFJackNo ratings yet
- Entering and Leaving The Traffic Separation SchemeDocument2 pagesEntering and Leaving The Traffic Separation SchemeAjay KumarNo ratings yet
- Topic 8 Chemicals in Industry: 8.1 AlloyDocument31 pagesTopic 8 Chemicals in Industry: 8.1 AlloyKonilia SualNo ratings yet
- 6936 PDFDocument2 pages6936 PDFSan Abelleta100% (2)