You might also like
- Atlas of Hybrid Imaging Sectional Anatomy for PET/CT, PET/MRI and SPECT/CT Vol. 2: Thorax Abdomen and Pelvis: Sectional Anatomy for PET/CT, PET/MRI and SPECT/CTFrom EverandAtlas of Hybrid Imaging Sectional Anatomy for PET/CT, PET/MRI and SPECT/CT Vol. 2: Thorax Abdomen and Pelvis: Sectional Anatomy for PET/CT, PET/MRI and SPECT/CTNo ratings yet
- Atlas of Hybrid Imaging Sectional Anatomy for PET/CT, PET/MRI and SPECT/CT Vol. 1: Brain and Neck: Sectional Anatomy for PET/CT, PET/MRI and SPECT/CTFrom EverandAtlas of Hybrid Imaging Sectional Anatomy for PET/CT, PET/MRI and SPECT/CT Vol. 1: Brain and Neck: Sectional Anatomy for PET/CT, PET/MRI and SPECT/CTNo ratings yet
- PET-CT for the Management of Cancer Patients: A Review of the Existing EvidenceFrom EverandPET-CT for the Management of Cancer Patients: A Review of the Existing EvidenceNo ratings yet
- Nuclear OncologyDocument33 pagesNuclear OncologyOvguOzenliNo ratings yet
- Hepatocellular Carcinoma: Review ArticleDocument13 pagesHepatocellular Carcinoma: Review ArticleAnnagiulia Gramenzi100% (2)
- Marjolin Ulcer POSTER (RSCM)Document1 pageMarjolin Ulcer POSTER (RSCM)Juli Jamnasi100% (1)
- Mucoepidermoid Carcinomaof The External Auditory Canal (Eac)Document4 pagesMucoepidermoid Carcinomaof The External Auditory Canal (Eac)IJAR JOURNALNo ratings yet
- Low Grade Glioma Treatment and PrognosisDocument5 pagesLow Grade Glioma Treatment and PrognosisDiana MitreaNo ratings yet
- Germ Cell TumoursDocument32 pagesGerm Cell Tumoursapi-3705046No ratings yet
- EAU ESUR ESTRO SIOG Guidelines On Prostate Cancer Large Text V2Document145 pagesEAU ESUR ESTRO SIOG Guidelines On Prostate Cancer Large Text V2DellaNo ratings yet
- 15 02 UpdateFetalTherapy 0Document59 pages15 02 UpdateFetalTherapy 0Ryan SadonoNo ratings yet
- ILRT Dr. Sarbani-1 PDFDocument48 pagesILRT Dr. Sarbani-1 PDFdurgesh kumar100% (1)
- Locally Advanced Breast CarcinomaDocument31 pagesLocally Advanced Breast Carcinomaapi-3701915100% (1)
- Ad en Om Yo SisDocument6 pagesAd en Om Yo SisMariaa EndahhNo ratings yet
- Recent Advances in Radiation Oncology: DR M Spoorthi Shelometh Department of Radiation OncologyDocument53 pagesRecent Advances in Radiation Oncology: DR M Spoorthi Shelometh Department of Radiation Oncologyspoorthi shelomethNo ratings yet
- Invasive Molar Pregnancy and MRI: What Every Radiologist Must KnowDocument51 pagesInvasive Molar Pregnancy and MRI: What Every Radiologist Must Knowmelchi santander go100% (1)
- Gynecological Brachytherapy GuideDocument8 pagesGynecological Brachytherapy GuideChristy Sitorus100% (1)
- Radiotherapy in Penile Carcinoma: Dr. Ayush GargDocument32 pagesRadiotherapy in Penile Carcinoma: Dr. Ayush GargMohammad Mahfujur RahmanNo ratings yet
- Management of The Pancreatic Remnant During Whipple OperationDocument4 pagesManagement of The Pancreatic Remnant During Whipple OperationYacine Tarik Aizel100% (1)
- F-18 NaFDocument47 pagesF-18 NaFLadipo Temitope AyodejiNo ratings yet
- Role For Radiation Therapy in MelanomaDocument13 pagesRole For Radiation Therapy in MelanomaHendry HuangNo ratings yet
- Dance - Davis Intubated Ureterotomy in A Child - 05202016Document27 pagesDance - Davis Intubated Ureterotomy in A Child - 05202016sirrfsNo ratings yet
- APBI Presentation: Accelerated Partial Breast Irradiation Techniques and OutcomesDocument20 pagesAPBI Presentation: Accelerated Partial Breast Irradiation Techniques and OutcomesRegan Ward HimeNo ratings yet
- Radiation Therapy Template for Gynecological CancerDocument12 pagesRadiation Therapy Template for Gynecological CancerarifpharmjuNo ratings yet
- Early Breast Cancer - From Screening To Multidisciplinary Management - 3E (PDF) (UnitedVRG)Document586 pagesEarly Breast Cancer - From Screening To Multidisciplinary Management - 3E (PDF) (UnitedVRG)Luciana Bruno MaiaNo ratings yet
- Quantec 02Document7 pagesQuantec 02onco100% (1)
- RadtheraDocument85 pagesRadtheraKotarou BokutoNo ratings yet
- Colorectal Cancer 1Document71 pagesColorectal Cancer 1Anupam SisodiaNo ratings yet
- Treatment Planning Heterogeneity Vs Homogeneity Lung ProjectDocument13 pagesTreatment Planning Heterogeneity Vs Homogeneity Lung Projectapi-299138743No ratings yet
- Management of Breast CancerDocument53 pagesManagement of Breast CancerGaoudam NatarajanNo ratings yet
- Tumor Markers: Bethy S. Hernowo Dept. of Pathology Anatomy UNPAD/ Hasan Sadikin Hospital BandungDocument31 pagesTumor Markers: Bethy S. Hernowo Dept. of Pathology Anatomy UNPAD/ Hasan Sadikin Hospital BandungDini DesmonaNo ratings yet
- The Lecture: "Tumours of The Mammary Gland."Document21 pagesThe Lecture: "Tumours of The Mammary Gland."top theNo ratings yet
- Molecular Carcinogenesis Endometrium PDFDocument7 pagesMolecular Carcinogenesis Endometrium PDFMelati HasnailNo ratings yet
- BIO 2 MergedDocument132 pagesBIO 2 Mergedsubham ghoshNo ratings yet
- Sc-PSMA-617 For Radiotheragnostics in Tandem With Lu-PSMA-617 - Preclinical Investigations in Comparison With Ga-PSMA-11 and Ga-PSMA-617Document10 pagesSc-PSMA-617 For Radiotheragnostics in Tandem With Lu-PSMA-617 - Preclinical Investigations in Comparison With Ga-PSMA-11 and Ga-PSMA-617Patricio AlfaroNo ratings yet
- NCCN Guideline RC v3 2022Document20 pagesNCCN Guideline RC v3 2022dony hendrawanNo ratings yet
- Breast Cancer in Women - A Narrative Literature ReviewDocument7 pagesBreast Cancer in Women - A Narrative Literature ReviewAnnie McSolsticeNo ratings yet
- Current Practice of Gleason Grading of Prostate Carcinoma: ReviewarticleDocument8 pagesCurrent Practice of Gleason Grading of Prostate Carcinoma: ReviewarticlecandiddreamsNo ratings yet
- Bethesda ScoreDocument7 pagesBethesda ScoreTiberiu BircaNo ratings yet
- Portfolio Pat 1Document18 pagesPortfolio Pat 1api-365835586No ratings yet
- DC HCCDocument12 pagesDC HCCSamah Abd ElhamidNo ratings yet
- 3DCRT Dan IMRTDocument57 pages3DCRT Dan IMRTMisael Christian100% (1)
- Comparison of Serum Microseminoprotein-Beta (MSMB) With Total Prostate Specific Antigen (TPSA) in The Diagnosis of Prostate Cancer in African MenDocument7 pagesComparison of Serum Microseminoprotein-Beta (MSMB) With Total Prostate Specific Antigen (TPSA) in The Diagnosis of Prostate Cancer in African MenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Principle of Chemotherapy Main PresentationDocument84 pagesPrinciple of Chemotherapy Main Presentationadekunle ajayiNo ratings yet
- 6 Sarcoma of The Uterus 2018 Clinical Gynecologic OncologyDocument10 pages6 Sarcoma of The Uterus 2018 Clinical Gynecologic OncologyMona HelouNo ratings yet
- Oncoplastic Breast SurgeryDocument27 pagesOncoplastic Breast SurgeryReem Amr El-DafrawiNo ratings yet
- Pictorial Essay: Multidetector CT Urography With Abdominal Compression and Three-Dimensional ReconstructionDocument13 pagesPictorial Essay: Multidetector CT Urography With Abdominal Compression and Three-Dimensional ReconstructionHarley Alejo MNo ratings yet
- Trimodality Therapy in Bladder CancerDocument12 pagesTrimodality Therapy in Bladder CancerStirNo ratings yet
- Esophageal CancerDocument34 pagesEsophageal CancerEzequiel GarciaNo ratings yet
- Basics of Radiation Therapy: Elaine M. Zeman, Eric C. Schreiber, and Joel E. TepperDocument33 pagesBasics of Radiation Therapy: Elaine M. Zeman, Eric C. Schreiber, and Joel E. TepperCeren AtahanNo ratings yet
- 05 Birads Us Reporting Acr 2013Document12 pages05 Birads Us Reporting Acr 2013shilacorinaNo ratings yet
- Spindle Cell LesionsDocument8 pagesSpindle Cell LesionsdrmanishsharmaNo ratings yet
- Oncology NotesDocument5 pagesOncology NotesLucky GomezNo ratings yet
- ASCO-SEP Medical Oncology Self-Evaluation Program, 7e by ASCODocument730 pagesASCO-SEP Medical Oncology Self-Evaluation Program, 7e by ASCOandrei vladNo ratings yet
- Management of Lung CancerDocument31 pagesManagement of Lung CancerPadmaj KulkarniNo ratings yet
- Diagnosis and Treatment of MelanomaDocument14 pagesDiagnosis and Treatment of MelanomaAnonymous Af24L7No ratings yet
- Understanding BrachytherapyDocument28 pagesUnderstanding Brachytherapyqwertu132No ratings yet
- Brachytherapy 140129094056 Phpapp02Document77 pagesBrachytherapy 140129094056 Phpapp02KAZOBA FRANCISNo ratings yet
- Pancreatic CancerDocument4 pagesPancreatic Cancersdf100% (1)
- The Better Alignment Performance of Tsal PDFDocument182 pagesThe Better Alignment Performance of Tsal PDFZafr O'ConnellNo ratings yet
- Journal of Computer Science and Informat PDFDocument376 pagesJournal of Computer Science and Informat PDFZafr O'ConnellNo ratings yet
- International Journal of Engineering Res PDFDocument14 pagesInternational Journal of Engineering Res PDFZafr O'ConnellNo ratings yet
- Questions For Part 3 - Topic: TransportationDocument39 pagesQuestions For Part 3 - Topic: TransportationZafr O'ConnellNo ratings yet
- Critical Lift Plan Each Piece of Partici PDFDocument1 pageCritical Lift Plan Each Piece of Partici PDFZafr O'ConnellNo ratings yet
- Lifting Code of PracticeDocument34 pagesLifting Code of Practiceakubestlah67% (3)
- Limiting LiabilityDocument9 pagesLimiting LiabilityZafr O'ConnellNo ratings yet
- Access Pearce 2293018 ProofDocument8 pagesAccess Pearce 2293018 ProofAndrei MihalacheNo ratings yet
- Free and Open-Source Control Software For 3-D Motion and ProcessingDocument12 pagesFree and Open-Source Control Software For 3-D Motion and Processingvadivel.km1527No ratings yet
- Airport ACEDocument51 pagesAirport ACEZafr O'ConnellNo ratings yet
- Low CostDocument9 pagesLow CostZafr O'ConnellNo ratings yet
- PET CT A New Imaging Technology in NucleDocument19 pagesPET CT A New Imaging Technology in NucleZafr O'ConnellNo ratings yet
- General Specification Painting and Galva PDFDocument19 pagesGeneral Specification Painting and Galva PDFZafr O'ConnellNo ratings yet
- Limiting LiabilityDocument9 pagesLimiting LiabilityZafr O'ConnellNo ratings yet
- Lifting Plan 0002 Rev 0A Procedure / Work Instruction / Job Note Page 1 of 15Document14 pagesLifting Plan 0002 Rev 0A Procedure / Work Instruction / Job Note Page 1 of 15Mohd Wirawan PutraNo ratings yet
- Lifting Code of PracticeDocument34 pagesLifting Code of Practiceakubestlah67% (3)
- TWO 2 X 500 MW MONG DUONG 1 THERMAL POWE PDFDocument61 pagesTWO 2 X 500 MW MONG DUONG 1 THERMAL POWE PDFZafr O'ConnellNo ratings yet
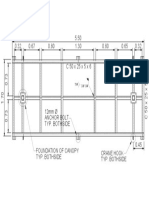
- Foundation plan for canopy with crane hook detailsDocument1 pageFoundation plan for canopy with crane hook detailsZafr O'ConnellNo ratings yet
- Company Contact and IKTVA Survey DetailsDocument21 pagesCompany Contact and IKTVA Survey DetailsZafr O'ConnellNo ratings yet
- MangoCultivation PDFDocument10 pagesMangoCultivation PDFcacsniteshNo ratings yet
- Piping ScheduleDocument4 pagesPiping ScheduleZafr O'ConnellNo ratings yet
- Norsok M CR 501r1Document19 pagesNorsok M CR 501r1Peter AllisonNo ratings yet
- Surface Preparation & Painting Procedure: List of ContentDocument14 pagesSurface Preparation & Painting Procedure: List of ContentZafr O'ConnellNo ratings yet
- Vdocuments - MX - Omni Flow Computer Manual PDFDocument57 pagesVdocuments - MX - Omni Flow Computer Manual PDFZafr O'ConnellNo ratings yet
- Technical SpecificationsDocument8 pagesTechnical SpecificationsZafr O'ConnellNo ratings yet
- BVM Catelogue New-2016 PDFDocument116 pagesBVM Catelogue New-2016 PDFOperation100% (1)
- PetroChina's Painting and Galvanizing SpecificationDocument19 pagesPetroChina's Painting and Galvanizing SpecificationZafr O'ConnellNo ratings yet
- General Specification for Painting and Surface PreparationDocument62 pagesGeneral Specification for Painting and Surface PreparationZafr O'ConnellNo ratings yet
- Unrep nwp04 01Document440 pagesUnrep nwp04 01Juckgrid Parnsomsakun100% (1)
- 411 PS1 2018 AnsDocument3 pages411 PS1 2018 AnsAlbertus MuheuaNo ratings yet
- Survey of Accounting 6th Edition Warren Solutions ManualDocument17 pagesSurvey of Accounting 6th Edition Warren Solutions Manualdevinsmithddsfzmioybeqr100% (19)
- Chem 6AL Syllabus Winter 2021Document5 pagesChem 6AL Syllabus Winter 2021John SmithNo ratings yet
- Civil Rights Web-QuestDocument5 pagesCivil Rights Web-Questapi-367833271No ratings yet
- Firebird Developer Guide Beta Delphi FiredacDocument162 pagesFirebird Developer Guide Beta Delphi FiredacDanilo CristianoNo ratings yet
- Members From The Vietnam Food AssociationDocument19 pagesMembers From The Vietnam Food AssociationMaiquynh DoNo ratings yet
- DSE2541 Data SheetDocument2 pagesDSE2541 Data SheetBERANGER DAVESNE DJOMALIA SIEWENo ratings yet
- BRI Divisions and Branches Level ReportDocument177 pagesBRI Divisions and Branches Level ReportCalvin Watulingas100% (1)
- The Irish Light 10Document28 pagesThe Irish Light 10Twinomugisha Ndinyenka RobertNo ratings yet
- Album China RayaDocument12 pagesAlbum China Rayaapitmelodi23No ratings yet
- Explosive Ordnance Disposal & Canine Group Regional Explosive Ordnance Disposal and Canine Unit 3Document1 pageExplosive Ordnance Disposal & Canine Group Regional Explosive Ordnance Disposal and Canine Unit 3regional eodk9 unit3No ratings yet
- FABM 1 Module by L. DimataloDocument109 pagesFABM 1 Module by L. Dimataloseraphinegod267No ratings yet
- Gold V Essex CCDocument11 pagesGold V Essex CCZACHARIAH MANKIRNo ratings yet
- 2.2 - T - Basic Negotiation Skill Vol. 1Document5 pages2.2 - T - Basic Negotiation Skill Vol. 1Siva 93No ratings yet
- Cut Nyak Dhien: Aceh's Legendary Resistance LeaderDocument5 pagesCut Nyak Dhien: Aceh's Legendary Resistance LeaderKhoerudin KhoerudinNo ratings yet
- T e 2552731 Describe The Creature Writing Worksheet - Ver - 2Document3 pagesT e 2552731 Describe The Creature Writing Worksheet - Ver - 2Minah ZamanNo ratings yet
- Bankruptcy Judge Imposes Sanctions On CounselDocument17 pagesBankruptcy Judge Imposes Sanctions On Counsel83jjmackNo ratings yet
- q2 Wk1 Worksheet1 Music8Document10 pagesq2 Wk1 Worksheet1 Music8Michie Maniego - GumanganNo ratings yet
- 07 - Toshkov (2016) Theory in The Research ProcessDocument29 pages07 - Toshkov (2016) Theory in The Research ProcessFerlanda LunaNo ratings yet
- Sun Life Takaful - 16062022Document8 pagesSun Life Takaful - 16062022PUI MUN CHANGNo ratings yet
- Human Rights EducationDocument149 pagesHuman Rights EducationLeonard MamergaNo ratings yet
- United States Court of Appeals, Third Circuit, 952 F.2d 742, 3rd Cir. (1991)Document22 pagesUnited States Court of Appeals, Third Circuit, 952 F.2d 742, 3rd Cir. (1991)Scribd Government DocsNo ratings yet
- Encounters 3Document4 pagesEncounters 3lgwqmsiaNo ratings yet
- Tugas B.INGGRIS ALANDocument4 pagesTugas B.INGGRIS ALANAlan GunawanNo ratings yet
- Moot Problem For ICA - NMIMS - June 2021Document3 pagesMoot Problem For ICA - NMIMS - June 2021AayushiNo ratings yet
- Ch01 Standard Methods and PractisesDocument44 pagesCh01 Standard Methods and PractisesUsman FarooqNo ratings yet
- Jim Beam Case Study Identify Roles and Organizational IssuesDocument4 pagesJim Beam Case Study Identify Roles and Organizational IssuesoluNo ratings yet
- Atty. Monna Lissa C. Monje-Viray: Are Hereto Attached As Annex "A" and "A-1"Document6 pagesAtty. Monna Lissa C. Monje-Viray: Are Hereto Attached As Annex "A" and "A-1"MarianoFloresNo ratings yet
- Hitachi - AssignmentDocument6 pagesHitachi - AssignmentPraveena IvanaNo ratings yet
- 333 Sapugay v. CADocument3 pages333 Sapugay v. CAJoshua Ejeil PascualNo ratings yet