You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Rebrand and Relaunch Hydrox CookiesDocument9 pagesRebrand and Relaunch Hydrox CookiesAruba KhanNo ratings yet
- Senarai Akta A MalaysiaDocument8 pagesSenarai Akta A MalaysiawswmadihiNo ratings yet
- KERATOCONUS Tanpa VideoDocument18 pagesKERATOCONUS Tanpa VideoMelia Budi AstutiNo ratings yet
- Congenital Retinal AnomaliesDocument92 pagesCongenital Retinal AnomaliesMelia Budi AstutiNo ratings yet
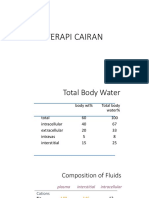
- Hipertonik Saline SolutionDocument12 pagesHipertonik Saline SolutionMelia Budi AstutiNo ratings yet
- Journal CorneaDocument6 pagesJournal CorneaMelia Budi AstutiNo ratings yet
- Journal CorneaDocument22 pagesJournal CorneaMelia Budi AstutiNo ratings yet
- Laporan Kasus BangsalDocument21 pagesLaporan Kasus BangsalMelia Budi AstutiNo ratings yet
- JurnalDocument15 pagesJurnalMelia Budi AstutiNo ratings yet
- 1 s2.0 S1878875019321898 Main PDFDocument4 pages1 s2.0 S1878875019321898 Main PDFMelia Budi AstutiNo ratings yet
- Uveitis5 160523124741Document38 pagesUveitis5 160523124741Melia Budi AstutiNo ratings yet
- JurnalDocument15 pagesJurnalMelia Budi AstutiNo ratings yet
- Wavefront A Text and AtlasDocument137 pagesWavefront A Text and AtlasMelia Budi AstutiNo ratings yet
- Leukocoria 180720093442Document34 pagesLeukocoria 180720093442Melia Budi AstutiNo ratings yet
- Corneal JournalDocument27 pagesCorneal JournalMelia Budi AstutiNo ratings yet
- CCFDocument7 pagesCCFMelia Budi AstutiNo ratings yet
- OctDocument45 pagesOctMelia Budi AstutiNo ratings yet
- CCFDocument2 pagesCCFMelia Budi AstutiNo ratings yet
- Solarte 2007Document13 pagesSolarte 2007Melia Budi AstutiNo ratings yet
- Persentase CairanDocument9 pagesPersentase CairanMelia Budi AstutiNo ratings yet
- Posterior SegmentDocument9 pagesPosterior SegmentMelia Budi AstutiNo ratings yet
- Persentase CairanDocument9 pagesPersentase CairanMelia Budi AstutiNo ratings yet
- Science Revision Sheet Year 7 Periodic 2Document5 pagesScience Revision Sheet Year 7 Periodic 2malknabih699No ratings yet
- Safety Competency TrainingDocument21 pagesSafety Competency TrainingsemajamesNo ratings yet
- Image Saving, Processing and Name Tagging Over SDTP Using Java ScriptDocument21 pagesImage Saving, Processing and Name Tagging Over SDTP Using Java Scriptsomnath banerjeeNo ratings yet
- Karakteristik Padi Gogo Lokal Yang Diber 325acbceDocument10 pagesKarakteristik Padi Gogo Lokal Yang Diber 325acbcemuhammad arjoniNo ratings yet
- Note 1-Estate Under AdministrationDocument8 pagesNote 1-Estate Under AdministrationNur Dina AbsbNo ratings yet
- 2 BA British and American Life and InstitutionsDocument3 pages2 BA British and American Life and Institutionsguest1957No ratings yet
- Wheel Loader wl56Document6 pagesWheel Loader wl56Shahzad AliNo ratings yet
- Name Caliber Base Penalties DMG Rate Clip Conceal Range CostDocument23 pagesName Caliber Base Penalties DMG Rate Clip Conceal Range CostLars Pedersen100% (1)
- Legal AgreementDocument2 pagesLegal AgreementMohd NadeemNo ratings yet
- RRR Budget Template 1Document4 pagesRRR Budget Template 1api-459388377No ratings yet
- Guideline Reading Diagnosis and Management of Pericardial DiseaseDocument87 pagesGuideline Reading Diagnosis and Management of Pericardial DiseaseMirza AlfiansyahNo ratings yet
- Synonyms, Antonyms, Spelling CorrectionsDocument10 pagesSynonyms, Antonyms, Spelling CorrectionsVenkateswara RasupalliNo ratings yet
- Fundamentals of Parenteral NutritionDocument4 pagesFundamentals of Parenteral NutritionankammaraoNo ratings yet
- My Slow Carb Diet Experience, Hacking With Four Hour BodyDocument37 pagesMy Slow Carb Diet Experience, Hacking With Four Hour BodyJason A. Nunnelley100% (2)
- 002 SM MP4054Document2,009 pages002 SM MP4054tranquangthuanNo ratings yet
- 2016 May Virginia Medical Law ReportDocument20 pages2016 May Virginia Medical Law ReportMichael DuntzNo ratings yet
- Deep Learning The Indus Script (Satish Palaniappan & Ronojoy Adhikari, 2017)Document19 pagesDeep Learning The Indus Script (Satish Palaniappan & Ronojoy Adhikari, 2017)Srini KalyanaramanNo ratings yet
- Maternal Newborn Nursing The Critical Components of Nursing Care 2nd Edition Durham Test BankDocument32 pagesMaternal Newborn Nursing The Critical Components of Nursing Care 2nd Edition Durham Test Bankalicenhan5bzm2z100% (24)
- Daftar PustakaDocument2 pagesDaftar PustakaBang UsopNo ratings yet
- Adult Patient InformationDocument1 pageAdult Patient Informationapi-521417613No ratings yet
- Chapter 18 Metric and Imperial Measures: Scheme of WorkDocument2 pagesChapter 18 Metric and Imperial Measures: Scheme of WorkrightwayNo ratings yet
- Hamlet Greek TragedyDocument21 pagesHamlet Greek TragedyJorge CanoNo ratings yet
- HR Awards PPT 2020 12.09.2020 FinalDocument64 pagesHR Awards PPT 2020 12.09.2020 FinalLolo OhwNo ratings yet
- Diss PDFDocument321 pagesDiss PDFAbdullah GhannamNo ratings yet
- 750-366 Hawk 1000 07 13 PDFDocument82 pages750-366 Hawk 1000 07 13 PDFAlexis CruzNo ratings yet
- LP Understanding The Writing ProcessDocument8 pagesLP Understanding The Writing Processargus.dump11No ratings yet
- Earth Art Michael Heizer The CityDocument2 pagesEarth Art Michael Heizer The Cityccxx09.cxNo ratings yet
- Rabindranath TagoreDocument13 pagesRabindranath TagoreVinay EkNo ratings yet