You might also like
- Pex 04 04 PDFDocument4 pagesPex 04 04 PDFshennie anteNo ratings yet
- Operation Whitecoat: Operation Whitecoat Was A Biodefense Medical Research Program CarriedDocument4 pagesOperation Whitecoat: Operation Whitecoat Was A Biodefense Medical Research Program Carriedshennie anteNo ratings yet
- Operation Whitecoat: Operation Whitecoat Was A Biodefense Medical Research Program CarriedDocument4 pagesOperation Whitecoat: Operation Whitecoat Was A Biodefense Medical Research Program Carriedshennie anteNo ratings yet
- Pex 04 04 PDFDocument4 pagesPex 04 04 PDFshennie anteNo ratings yet
- Pex 04 04 PDFDocument4 pagesPex 04 04 PDFshennie anteNo ratings yet
- Tuskegee Syphilis ExperimentDocument15 pagesTuskegee Syphilis Experimentshennie anteNo ratings yet
- Totskoye Nuclear Exercise: HistoryDocument5 pagesTotskoye Nuclear Exercise: Historyshennie anteNo ratings yet
- (PhysioEX Chapter 4 Exercise 2) PEX-04-02 - Steemit PDFDocument5 pages(PhysioEX Chapter 4 Exercise 2) PEX-04-02 - Steemit PDFshennie ante100% (1)
- Nazi Human ExperimentationDocument11 pagesNazi Human Experimentationshennie anteNo ratings yet
- Ohio State Prison Inmates: CommentsDocument2 pagesOhio State Prison Inmates: Commentsshennie anteNo ratings yet
- Guatemala Syphilis Experiment PDFDocument4 pagesGuatemala Syphilis Experiment PDFshennie anteNo ratings yet
- A History of Public Health - Rosen 1993Document441 pagesA History of Public Health - Rosen 1993Eder Ortiz Roca100% (5)
- Guatemala Syphilis Experiment PDFDocument4 pagesGuatemala Syphilis Experiment PDFshennie anteNo ratings yet
- 4613ijsea03 PDFDocument10 pages4613ijsea03 PDFshennie anteNo ratings yet
- Labmed32 0368Document8 pagesLabmed32 0368shennie anteNo ratings yet
- Pex 04 02Document5 pagesPex 04 02shennie anteNo ratings yet
- (PhysioEX Chapter 4 Exercise 2) PEX-04-02 - Steemit PDFDocument5 pages(PhysioEX Chapter 4 Exercise 2) PEX-04-02 - Steemit PDFshennie ante100% (1)
- Pex 11Document4 pagesPex 11shennie anteNo ratings yet
- A Mysterious Case of A Breast Lump in A WomanDocument3 pagesA Mysterious Case of A Breast Lump in A Womanshennie anteNo ratings yet
- Pex 04 03Document4 pagesPex 04 03shennie anteNo ratings yet
- (PhysioEX Chapter 11 Exercise 5) PEX-11-05 - SteemitDocument4 pages(PhysioEX Chapter 11 Exercise 5) PEX-11-05 - Steemitshennie anteNo ratings yet
- (PhysioEX Chapter 4 Exercise 2) PEX-04-02 - Steemit PDFDocument5 pages(PhysioEX Chapter 4 Exercise 2) PEX-04-02 - Steemit PDFshennie ante100% (1)
- A Brief History of VaccinationDocument1 pageA Brief History of Vaccinationshennie anteNo ratings yet
- CHAPTER 16 Digestive SystemDocument4 pagesCHAPTER 16 Digestive Systemshennie anteNo ratings yet
- Chapter 25 Ear PicsDocument12 pagesChapter 25 Ear Picsshennie anteNo ratings yet
- MICHIGAN Duodenum, Pancreas and Abdominal AortaDocument21 pagesMICHIGAN Duodenum, Pancreas and Abdominal Aortashennie anteNo ratings yet
- A Brief History of VaccinationDocument1 pageA Brief History of Vaccinationshennie anteNo ratings yet
- A Brief History of VaccinationDocument1 pageA Brief History of Vaccinationshennie anteNo ratings yet
- Chapter 1 Biochemistry and MedicineDocument1 pageChapter 1 Biochemistry and Medicineshennie anteNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Care of Older Adult Lecture (Reviewer)Document13 pagesCare of Older Adult Lecture (Reviewer)Antoinette PeleñaNo ratings yet
- Medicaid in Long Term CareDocument7 pagesMedicaid in Long Term Carerara100% (1)
- Formal Long Term Care: Informal Caregivers' Subjective Well Being and Service UtilizationDocument240 pagesFormal Long Term Care: Informal Caregivers' Subjective Well Being and Service UtilizationCHEE KOK SENGNo ratings yet
- Department of Health - Use, Collection, and Reporting of Infection Control DataDocument58 pagesDepartment of Health - Use, Collection, and Reporting of Infection Control DataNews10NBCNo ratings yet
- March 13, 2015 Strathmore TimesDocument36 pagesMarch 13, 2015 Strathmore TimesStrathmore TimesNo ratings yet
- Resume of GhummrichDocument1 pageResume of Ghummrichapi-27520385No ratings yet
- Improving AccessDocument67 pagesImproving AccessRiza EvantinaNo ratings yet
- Individualized Nutrition ApproachesDocument12 pagesIndividualized Nutrition ApproachesAndréia OliveiraNo ratings yet
- Mmi Caregiving Costs Working CaregiversDocument26 pagesMmi Caregiving Costs Working CaregiversSuman KondojuNo ratings yet
- Money Follow The Patient RFPDocument40 pagesMoney Follow The Patient RFPJonathan LaMantiaNo ratings yet
- COVID MoveFromLongTermCareDocument5 pagesCOVID MoveFromLongTermCareinforumdocsNo ratings yet
- Compendium - Better Government Competition 2017Document34 pagesCompendium - Better Government Competition 2017Pioneer InstituteNo ratings yet
- Consumer Guide To Medicaid PlanningDocument28 pagesConsumer Guide To Medicaid PlanningChristine NohNo ratings yet
- VISN16 Market RecommendationDocument58 pagesVISN16 Market RecommendationKALB DIGITALNo ratings yet
- 4 - OHRS - V10 - 2 - Chapter 4 - 2018 - 04 - 01 FinalDocument29 pages4 - OHRS - V10 - 2 - Chapter 4 - 2018 - 04 - 01 FinaljanNo ratings yet
- Document PDFDocument16 pagesDocument PDFtoni_yousf2418No ratings yet
- Insurance Japan Long TermDocument9 pagesInsurance Japan Long TermutisariNo ratings yet
- Ontario Jurisprudence Exam Notes - Ontario Drug Benefit Act (2/2)Document4 pagesOntario Jurisprudence Exam Notes - Ontario Drug Benefit Act (2/2)Herodotus100% (5)
- CLI - 2012 07 18 - Senior and Older Adult Village ModelsDocument63 pagesCLI - 2012 07 18 - Senior and Older Adult Village ModelsYelda Kızıldağ ÖzdemirliNo ratings yet
- US Internal Revenue Service: I1099ltc 07Document2 pagesUS Internal Revenue Service: I1099ltc 07IRSNo ratings yet
- Leumit Passport To HealthDocument13 pagesLeumit Passport To HealthEnglishAccessibilityNo ratings yet
- An Overview of Systems For Providing Integrated and Comprehensive Care For Older People in JapanDocument12 pagesAn Overview of Systems For Providing Integrated and Comprehensive Care For Older People in JapanimidazolaNo ratings yet
- Long Term LivingDocument168 pagesLong Term LivingJohann Victorious-Redd SmithNo ratings yet
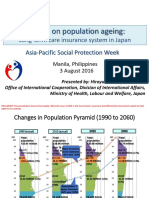
- APSP - Session 9A - Hiroyuki Yamaya - MHLWDocument8 pagesAPSP - Session 9A - Hiroyuki Yamaya - MHLWKristine PresbiteroNo ratings yet
- Long Term Care Insurance Shoppers Guide 10/2012Document72 pagesLong Term Care Insurance Shoppers Guide 10/2012beattherateNo ratings yet
- Arpa Planning Proposal FinalDocument10 pagesArpa Planning Proposal FinalTitus WuNo ratings yet
- Challenges in Long-Term Care in Europe: A Study of National Policies 2018Document66 pagesChallenges in Long-Term Care in Europe: A Study of National Policies 2018Alexandru ConstantinNo ratings yet
- Ebook PDF Dimensions of Long Term Care Management An Introduction Second Edition PDFDocument42 pagesEbook PDF Dimensions of Long Term Care Management An Introduction Second Edition PDFlatasha.ahern217100% (34)
- Financial Statement Analysis of TCS and INFOSYSDocument43 pagesFinancial Statement Analysis of TCS and INFOSYSRitwik Subudhi100% (1)
- General Hospital Literature Review - Zemran, Abdisa, LensaDocument40 pagesGeneral Hospital Literature Review - Zemran, Abdisa, Lensazemran girmaNo ratings yet