You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Morbus Hansen: Dr. Citra Primanita, SP - KKDocument16 pagesMorbus Hansen: Dr. Citra Primanita, SP - KKTitisNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Type 1 Diabetes MellitusDocument18 pagesType 1 Diabetes MellitusTitisNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- K47. Vit D and HiperinsulinDocument15 pagesK47. Vit D and HiperinsulinTitisNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Short Stature or StuntingDocument16 pagesShort Stature or StuntingTitisNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Corneal Ulcers WHO PDFDocument36 pagesCorneal Ulcers WHO PDFAlifa FaradillaNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Kelainan Saraf KongenitalDocument35 pagesKelainan Saraf KongenitalTitisNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Disease Occurrence ComparisonDocument12 pagesDisease Occurrence ComparisonTitisNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Pathology of Joints & Related Structure (Dr. Dody) SendiDocument30 pagesPathology of Joints & Related Structure (Dr. Dody) SendiTitisNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
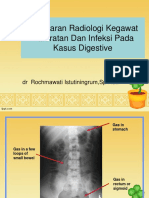
- K29 - Radiologi Blok Digestive 2015Document117 pagesK29 - Radiologi Blok Digestive 2015NininghrNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Short Stature or StuntingDocument16 pagesShort Stature or StuntingTitisNo ratings yet
- Psikologi BencanaDocument19 pagesPsikologi BencanaTitisPudyatikaDestyaAndiraNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Epidemiology MASDocument1 pageEpidemiology MASTitisNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- DFSGDFGDFDocument60 pagesDFSGDFGDFMada Dwi HariNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Muscoletalsceletal InjuriesDocument15 pagesMuscoletalsceletal InjuriesTitisNo ratings yet
- Manual InternDocument136 pagesManual InternalvinatNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Pathogenesis of Bacterial InfectionDocument35 pagesPathogenesis of Bacterial InfectionDiyantoro NyoNo ratings yet
- Cefuroxime, Celecoxib, ChloridineDocument2 pagesCefuroxime, Celecoxib, ChloridinekrizzywhizzyNo ratings yet
- Corona Virus (Covid19) : The Grim RealityDocument6 pagesCorona Virus (Covid19) : The Grim RealityGenevieve GayosoNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Disorders of Coagulation FactorsDocument35 pagesDisorders of Coagulation FactorsMelesNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- NCP PryllDocument6 pagesNCP PryllpjcolitaNo ratings yet
- Soal PTS Bahasa Inggris Kelas XiDocument3 pagesSoal PTS Bahasa Inggris Kelas XiHafiz AriNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Prevenção Secundária Avc Isquêmico - Guideline 2022Document41 pagesPrevenção Secundária Avc Isquêmico - Guideline 2022Felipe Stoquetti de AbreuNo ratings yet
- Aleukemic LeukemiaDocument3 pagesAleukemic LeukemialilisNo ratings yet
- Department of Obstetrics and Gynecology FinalDocument42 pagesDepartment of Obstetrics and Gynecology Finalkremlin23455No ratings yet
- Internal Medicine Clinical Treatment Guidelines 9-10-2012 1Document264 pagesInternal Medicine Clinical Treatment Guidelines 9-10-2012 1ursula_ursulaNo ratings yet
- Berikut Ini Macam Macam Penyakit Dan Istilah MedisDocument24 pagesBerikut Ini Macam Macam Penyakit Dan Istilah MedisIis Izy IssooNo ratings yet
- Practical's OrthopaedicDocument11 pagesPractical's Orthopaedicranamiraj731No ratings yet
- DSM IIDocument136 pagesDSM IIfarleyknight100% (17)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Creutzfeldt-Jakob Disease (CJD)Document10 pagesCreutzfeldt-Jakob Disease (CJD)Thicc ManNo ratings yet
- CV of BaifengZhang.2023Document3 pagesCV of BaifengZhang.2023Baifeng ZhangNo ratings yet
- Rheumatoid Arthritis Drug StudyDocument2 pagesRheumatoid Arthritis Drug StudyChristaNo ratings yet
- Assessment Diagnosis Objectives of Care Intervention Rationale Evaluation Difficulty of Breathing (Rapid and Shallow)Document1 pageAssessment Diagnosis Objectives of Care Intervention Rationale Evaluation Difficulty of Breathing (Rapid and Shallow)Jamaica Leslie NovenoNo ratings yet
- Normal Digestion / Absorption of FatDocument5 pagesNormal Digestion / Absorption of FatMarc Michael Dela CruzNo ratings yet
- D. Nursing Care Plan: Chronic Pain Related ToDocument2 pagesD. Nursing Care Plan: Chronic Pain Related ToReinette LastrillaNo ratings yet
- Lecture Schedule-3rd Year-Sem I-2023 & 2024Document2 pagesLecture Schedule-3rd Year-Sem I-2023 & 2024Jonathan AustinNo ratings yet
- Physiotherapy in Leprosy: Presented byDocument20 pagesPhysiotherapy in Leprosy: Presented byvyomphysio201050% (2)
- ParalysisDocument4 pagesParalysissakuraleeshaoranNo ratings yet
- Wellen EcgDocument9 pagesWellen EcgElokNo ratings yet
- Midterm Activity ScitechDocument3 pagesMidterm Activity ScitechKean KaiNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Mark Klimek Review DelegationDocument6 pagesMark Klimek Review DelegationKarima Jones100% (1)
- Diagnosis of Brown Sequard SyndromeDocument3 pagesDiagnosis of Brown Sequard SyndromeOktavianus PrayitnoNo ratings yet
- SPC For Health Care Providers - Ivermax - Kaplet 12 MG - Ivermektin - DKL2107926604A1 - 2021 - 0 - 0Document4 pagesSPC For Health Care Providers - Ivermax - Kaplet 12 MG - Ivermektin - DKL2107926604A1 - 2021 - 0 - 0Timothy OlsonNo ratings yet
- Acute Myeloid LeukemiaDocument1 pageAcute Myeloid LeukemiaAlleah Salbo KepusNo ratings yet
- Andaman Fever A New EntityDocument6 pagesAndaman Fever A New EntitySheepu SharmaNo ratings yet