You might also like
- Health Questionnaire Form (HQF)Document1 pageHealth Questionnaire Form (HQF)salmanNo ratings yet
- Crewsure Claim Form (XLCatlin) 1.3Document2 pagesCrewsure Claim Form (XLCatlin) 1.3Andrei Belehuzi0% (1)
- Cholesterol Mortality ChartDocument1 pageCholesterol Mortality ChartTms ArnNo ratings yet
- Fluid & ElectrolyteDocument26 pagesFluid & Electrolytesanjana bhatia100% (1)
- Proposal Form Ashakiran PDFDocument6 pagesProposal Form Ashakiran PDFSreejith Rajendran PillaiNo ratings yet
- Family FLoater FormDocument6 pagesFamily FLoater FormSantosh KodereNo ratings yet
- Proposal Form New India Floater Mediclaim Policy 21012020 - 1Document6 pagesProposal Form New India Floater Mediclaim Policy 21012020 - 1aj iseNo ratings yet
- Mediclaim 2012 Proposal FormDocument6 pagesMediclaim 2012 Proposal FormgaurnityanandaNo ratings yet
- Proposal Form New India Mediclaim Policy 01102021Document6 pagesProposal Form New India Mediclaim Policy 01102021abcdefabcNo ratings yet
- Proposal Form New India Mediclaim PolicyDocument6 pagesProposal Form New India Mediclaim PolicyPavan Kumar NarbolikarNo ratings yet
- NSTUMP - Proposal FormDocument7 pagesNSTUMP - Proposal FormJagadeesh MaheshNo ratings yet
- The New India Assurance Company Limited: Head Office: 87, M G Road, Fort, Mumbai-400001 Mediclaim Insurance Proposal FormDocument6 pagesThe New India Assurance Company Limited: Head Office: 87, M G Road, Fort, Mumbai-400001 Mediclaim Insurance Proposal FormChirantan BuchNo ratings yet
- Proposal Form For New India Premier MediclaimDocument6 pagesProposal Form For New India Premier MediclaimAnonymous 95dlTK1McNo ratings yet
- Proof of Loss Form for Study USA HealthCareDocument2 pagesProof of Loss Form for Study USA HealthCareborn2bewildNo ratings yet
- Saral Suraksha Bima, Plan - Preposal Form - v1Document3 pagesSaral Suraksha Bima, Plan - Preposal Form - v1rajeshNo ratings yet
- Star Health Insurance Proposal FormDocument2 pagesStar Health Insurance Proposal FormBhaktha SinghNo ratings yet
- NPMP Parivar Proposal FormDocument8 pagesNPMP Parivar Proposal Formpradip nathujiNo ratings yet
- Parivar Proposal FormDocument10 pagesParivar Proposal FormHANSDA DHIRENDRANATHANNo ratings yet
- IHP Proposal FormDocument9 pagesIHP Proposal FormDeepakNo ratings yet
- Kutumb Swasthya Bima Policy - GroupDocument4 pagesKutumb Swasthya Bima Policy - Grouprohit kakkarNo ratings yet
- SBIL - Health QuestionnaireDocument2 pagesSBIL - Health QuestionnaireKrishna GBNo ratings yet
- Ti Claim FormDocument8 pagesTi Claim FormHihiNo ratings yet
- BSIB GHS Claim FormDocument3 pagesBSIB GHS Claim FormmuhsinmohammedNo ratings yet
- OMP Proposal Form (Business and Holiday) PDFDocument6 pagesOMP Proposal Form (Business and Holiday) PDFdhananjay shuklaNo ratings yet
- PRP 23 7000179227PRP 23 7000179227Document7 pagesPRP 23 7000179227PRP 23 7000179227Arvind KumarNo ratings yet
- MediRaksha Proposal FormDocument4 pagesMediRaksha Proposal FormNarayana MugalurNo ratings yet
- Head Office: 87, M G Road, Fort, Mumbai-400001: I. II - CLAIM NO.Document5 pagesHead Office: 87, M G Road, Fort, Mumbai-400001: I. II - CLAIM NO.gaddipati_ramuNo ratings yet
- National Insurance Varistha Proposal FormDocument5 pagesNational Insurance Varistha Proposal FormAnirBanerjee0% (1)
- PP CformDocument4 pagesPP CformHihiNo ratings yet
- Important:: CIGNA Group InsuranceDocument2 pagesImportant:: CIGNA Group InsuranceLoganBohannonNo ratings yet
- FB ClaimDocument14 pagesFB ClaimHihiNo ratings yet
- Claimant Statement With ETF Mandate FormDocument6 pagesClaimant Statement With ETF Mandate FormKishan GarhtiyaNo ratings yet
- FB Pregnancy-ComplicationDocument19 pagesFB Pregnancy-ComplicationHihiNo ratings yet
- National Insurance Company LimitedDocument4 pagesNational Insurance Company Limitedkaransandesara777No ratings yet
- Domestic Maid Claim FormDocument4 pagesDomestic Maid Claim FormHihiNo ratings yet
- CC Stroke NewDocument12 pagesCC Stroke NewHihiNo ratings yet
- Form 300Document8 pagesForm 300Sachin SharmaNo ratings yet
- Hospital Cash Claim FormDocument5 pagesHospital Cash Claim FormVivek UmbreNo ratings yet
- Enrolment form employee benefitsDocument1 pageEnrolment form employee benefitsCalleja Jemimah Rose AristokiNo ratings yet
- PH IcformDocument4 pagesPH IcformHihiNo ratings yet
- OVHC Claim Form 102017 PDFDocument3 pagesOVHC Claim Form 102017 PDFtarmudiNo ratings yet
- Medical Insurance Proposal Form SummaryDocument4 pagesMedical Insurance Proposal Form SummaryReet HansahNo ratings yet
- Mumbai Claim FormDocument5 pagesMumbai Claim FormsunsangraNo ratings yet
- GMHP Claim Form - Online PDFDocument4 pagesGMHP Claim Form - Online PDFSalem AmraneNo ratings yet
- Hospitalization Claim Form DetailsDocument6 pagesHospitalization Claim Form DetailspritamNo ratings yet
- GMC Claim Form How To File A ClaimDocument4 pagesGMC Claim Form How To File A ClaimtweetknotNo ratings yet
- Easy Health Proposal FormDocument5 pagesEasy Health Proposal Formomshanker44No ratings yet
- Happy Family FloaterformDocument5 pagesHappy Family FloaterformWealthMitra Financial ServicesNo ratings yet
- NTUC Claim FormDocument5 pagesNTUC Claim FormHihiNo ratings yet
- Marsh PNG Medicare CLAIM FORMDocument3 pagesMarsh PNG Medicare CLAIM FORMKaitaMahn100% (1)
- Attending Physicians Statement Crisis Cover Muscular Dystrophy - 041222Document2 pagesAttending Physicians Statement Crisis Cover Muscular Dystrophy - 041222laraNo ratings yet
- Form ID-01: A. Personal DetailsDocument4 pagesForm ID-01: A. Personal DetailsNarendra BejNo ratings yet
- Good Health DeclarationDocument2 pagesGood Health DeclarationPraharshit GorripatyNo ratings yet
- Sample: Ab Health HameshaDocument4 pagesSample: Ab Health HameshaVikas MehtaNo ratings yet
- Total and Permanent Disability Claim FormDocument2 pagesTotal and Permanent Disability Claim FormPrashob SugathanNo ratings yet
- PM OthersDocument35 pagesPM OthersHihiNo ratings yet
- ROYAL SUNDARAM HEALTH CLAIM FORMDocument3 pagesROYAL SUNDARAM HEALTH CLAIM FORMகமலேஷ் குமார்No ratings yet
- HDFC ERGO General Insurance Company Limited: Easy Health - Proposal FormDocument8 pagesHDFC ERGO General Insurance Company Limited: Easy Health - Proposal FormDilip ManiyarNo ratings yet
- Doctor's Indemnity Proposal FormDocument5 pagesDoctor's Indemnity Proposal FormPriyank guptaNo ratings yet
- Sukshma Hospi CashDocument4 pagesSukshma Hospi CashAdemuyiwa OlaniyiNo ratings yet
- A Guide for Medical Case Managers: Stop Loss Insurance for Medical ProfessionalsFrom EverandA Guide for Medical Case Managers: Stop Loss Insurance for Medical ProfessionalsNo ratings yet
- Magnetic S1Document2 pagesMagnetic S1Hemraj SonarNo ratings yet
- Recoil Technical Catalogue 2018Document112 pagesRecoil Technical Catalogue 2018Marsal CMNo ratings yet
- Powergrip Gt3 Design Manual Us January 2014Document199 pagesPowergrip Gt3 Design Manual Us January 2014Hemraj SonarNo ratings yet
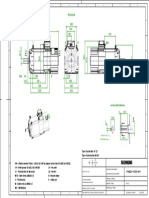
- Asynchron-Servomotor front viewDocument1 pageAsynchron-Servomotor front viewHemraj SonarNo ratings yet
- RRB Cen 03-2018Document63 pagesRRB Cen 03-2018NDTVNo ratings yet
- Is 808-1989 Steel TableDocument24 pagesIs 808-1989 Steel TableAtul Kumar Engineer86% (28)
- Seminar ReportDocument16 pagesSeminar ReportHemraj SonarNo ratings yet
- Anemia.: Seminar OnDocument24 pagesAnemia.: Seminar OnAlma Susan100% (1)
- Herbal - Medicines - in - The - Treatment of Mental IllnessesDocument12 pagesHerbal - Medicines - in - The - Treatment of Mental IllnessesFarash farshiNo ratings yet
- Physio. D. Suroor. L1. BloodDocument24 pagesPhysio. D. Suroor. L1. Bloodزين العابدين محمد عويشNo ratings yet
- Assessment Report On Ginkgo Biloba L., Folium DDocument120 pagesAssessment Report On Ginkgo Biloba L., Folium DMiroslav IlicNo ratings yet
- CT ReportsDocument3 pagesCT Reportssukesh sukesh100% (1)
- Snake Bite Monitoring and TreatmentDocument66 pagesSnake Bite Monitoring and TreatmentedfZSEADFsfsafafNo ratings yet
- ELIMINATION ASSESSMENTDocument7 pagesELIMINATION ASSESSMENTNareswari KenitenNo ratings yet
- Understanding Amnestic DisordersDocument31 pagesUnderstanding Amnestic DisordersKhadija ArshadNo ratings yet
- NAlduaij Kuwait Snakes MENATOX2009Document19 pagesNAlduaij Kuwait Snakes MENATOX2009dave fowler0% (1)
- Fluid Management in The Critically Ill: Jean-Louis VincentDocument6 pagesFluid Management in The Critically Ill: Jean-Louis VincentLucas MontanhaNo ratings yet
- Geriatric Dentistry NewDocument45 pagesGeriatric Dentistry NewRahul SinghNo ratings yet
- XXXDocument134 pagesXXXrhlzuraNo ratings yet
- Bishaw Assigment of GI DisorderDocument98 pagesBishaw Assigment of GI DisorderRas Siko SafoNo ratings yet
- Curcumin Role in ParaproteinemiaDocument18 pagesCurcumin Role in ParaproteinemiaINDIRAKALYANINo ratings yet
- Ugm - Hipertensi PulmoDocument28 pagesUgm - Hipertensi PulmoAfif RiondiNo ratings yet
- Output 1 Electrolytes - DraftDocument16 pagesOutput 1 Electrolytes - Draftallanrnmanaloto100% (1)
- Philippine Nursing Licensure ExaminationDocument32 pagesPhilippine Nursing Licensure ExaminationVera100% (1)
- Drug StudyDocument5 pagesDrug StudyKenneth Narciso PerezNo ratings yet
- Nursing Test 2 (NP Iii)Document19 pagesNursing Test 2 (NP Iii)Yuxin LiuNo ratings yet
- DermatopatologiDocument117 pagesDermatopatologiSariNo ratings yet
- Tweets @oketoast: @markccrowleyDocument2 pagesTweets @oketoast: @markccrowleyOkefenokee Toastmasters ClubNo ratings yet
- HirudotherapyDocument2 pagesHirudotherapyshirajshah100% (2)
- Heart RhythmDocument68 pagesHeart RhythmMwanja MosesNo ratings yet
- ValuCare Application Form112116Document2 pagesValuCare Application Form112116Lea JoanaNo ratings yet
- Blood Lecture 2023fallDocument18 pagesBlood Lecture 2023falldodomrmr205No ratings yet
- Epinephrine DrugStudy WWW Rnpedia ComDocument4 pagesEpinephrine DrugStudy WWW Rnpedia ComIrish LigayaNo ratings yet
- Managing Health in The Aluminium IndustryDocument346 pagesManaging Health in The Aluminium IndustryWellfro100% (1)
- The Neurological Exam: Mental Status ExaminationDocument13 pagesThe Neurological Exam: Mental Status ExaminationShitaljit IromNo ratings yet