You might also like
- Shanghairanking'S Global Ranking of Academic Subjects 2019 - Clinical MedicineDocument13 pagesShanghairanking'S Global Ranking of Academic Subjects 2019 - Clinical MedicineNgh33No ratings yet
- 4 5782675776138642694 PDFDocument1 page4 5782675776138642694 PDFNgh33No ratings yet
- Application For A Residence Permit in Denmark in Order To Obtain A Danish Authorisation or As A VolunteerDocument8 pagesApplication For A Residence Permit in Denmark in Order To Obtain A Danish Authorisation or As A VolunteerNgh33No ratings yet
- Dentistry: (For International Students)Document2 pagesDentistry: (For International Students)Ngh33No ratings yet
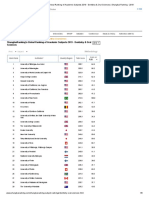
- Shanghairanking'S Global Ranking of Academic Subjects 2019 - Dentistry & Oral SciencesDocument8 pagesShanghairanking'S Global Ranking of Academic Subjects 2019 - Dentistry & Oral SciencesNgh33No ratings yet
- Gangadharan 2009Document11 pagesGangadharan 2009Ngh33No ratings yet
- Isrn Psychiatry2013-621453Document7 pagesIsrn Psychiatry2013-621453Ngh33No ratings yet
- Darley 1982Document7 pagesDarley 1982Ngh33No ratings yet
- Torner 2016Document6 pagesTorner 2016Ngh33No ratings yet
- 2323 2329 Art. 3092 PDFDocument7 pages2323 2329 Art. 3092 PDFNgh33No ratings yet
- Nagy 2006Document11 pagesNagy 2006Ngh33No ratings yet
- 10 1111@j 1468-3083 2012 04658 XDocument4 pages10 1111@j 1468-3083 2012 04658 XNgh33No ratings yet
- Wong 2015Document3 pagesWong 2015Ngh33No ratings yet
- Torner 2016Document6 pagesTorner 2016Ngh33No ratings yet
- Gonzalez Iglesias2008Document10 pagesGonzalez Iglesias2008Ngh33No ratings yet
- Trisno 2015Document1 pageTrisno 2015Ngh33No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Assignment 2 Management Perspective Son Leadership MotivationDocument14 pagesAssignment 2 Management Perspective Son Leadership MotivationHoneyVasudevNo ratings yet
- GutsDocument552 pagesGutsroparts cluj100% (1)
- Doyennés Et Granges de L'abbaye de Cluny (A. Guerreau)Document45 pagesDoyennés Et Granges de L'abbaye de Cluny (A. Guerreau)theseus11No ratings yet
- Chinese MedicineDocument16 pagesChinese MedicineTrisNo ratings yet
- Physics Unit 3 Practice Test Dynamics5Document5 pagesPhysics Unit 3 Practice Test Dynamics5StephanieNo ratings yet
- Buzan, Barry - Security, The State, The 'New World Order' & BeyondDocument15 pagesBuzan, Barry - Security, The State, The 'New World Order' & Beyondyossara26100% (3)
- CH 6 Answers (All) PDFDocument29 pagesCH 6 Answers (All) PDFAhmed SideegNo ratings yet
- Brochure Delegation Training For LeadersDocument6 pagesBrochure Delegation Training For LeadersSupport ALProgramsNo ratings yet
- Jim 1000 RC 3Document33 pagesJim 1000 RC 3singingblueeNo ratings yet
- 1 Kane Equations - Example 1Document8 pages1 Kane Equations - Example 1Khisbullah HudhaNo ratings yet
- Chemistry Module 3Document14 pagesChemistry Module 3MASHNo ratings yet
- Research Proposal Sample OutlineDocument17 pagesResearch Proposal Sample OutlineGuidance and Counseling OfficeNo ratings yet
- Fastener Torque Charts: Phone: 1-800-558-2808 Fax: 1-800-553-8769Document2 pagesFastener Torque Charts: Phone: 1-800-558-2808 Fax: 1-800-553-8769KOMATSU SHOVELNo ratings yet
- Obat Keras N0vember 2021Document137 pagesObat Keras N0vember 2021antonNo ratings yet
- School Earthquake Preparedness Evaluation FormDocument2 pagesSchool Earthquake Preparedness Evaluation FormAdrin Mejia75% (4)
- Examples Week1 CompressDocument6 pagesExamples Week1 CompressAngel HuitradoNo ratings yet
- Blackrock Methods of Delay AnalysisDocument36 pagesBlackrock Methods of Delay AnalysisAhmed MoubarkNo ratings yet
- NewspaperDocument2 pagesNewspaperbro nabsNo ratings yet
- Kibera Mirror JULYDocument8 pagesKibera Mirror JULYvincent achuka maisibaNo ratings yet
- Hal Foster Vision and Visuality Discussions in Contemporary Culture PDFDocument75 pagesHal Foster Vision and Visuality Discussions in Contemporary Culture PDFEd GomesNo ratings yet
- FPI - Study Permit Application GuideDocument9 pagesFPI - Study Permit Application GuideKian Mark DarioNo ratings yet
- 11 My Immigration Story - Tan Le QuestionsDocument3 pages11 My Immigration Story - Tan Le QuestionsMallika Nand NairNo ratings yet
- What Is StevedoringDocument10 pagesWhat Is StevedoringMinhaj KmNo ratings yet
- TM GUIDE (Basic Competencies)Document19 pagesTM GUIDE (Basic Competencies)Emelito T. ColentumNo ratings yet
- Jahnteller Effect Unit 3 2017Document15 pagesJahnteller Effect Unit 3 2017Jaleel BrownNo ratings yet
- Dania - 22 - 12363 - 1-Lecture 2 Coordinate System-Fall 2015Document34 pagesDania - 22 - 12363 - 1-Lecture 2 Coordinate System-Fall 2015erwin100% (1)
- LP Addition of PolynomialsDocument5 pagesLP Addition of PolynomialsJolina Bagwisa LptNo ratings yet
- Report Text The Duck Billed Platypus: (Ornithorhynchus Anatinus)Document2 pagesReport Text The Duck Billed Platypus: (Ornithorhynchus Anatinus)Lilis IndriyaniNo ratings yet
- Case 07-53: #REF! #REF! #REF! #REF! #REF!Document6 pagesCase 07-53: #REF! #REF! #REF! #REF! #REF!saad bin sadaqatNo ratings yet
- What Is E-CollaborationDocument7 pagesWhat Is E-CollaborationToumba LimbreNo ratings yet