You might also like
- CPG Uti PDFDocument7 pagesCPG Uti PDFhellokathyyyyyyNo ratings yet
- CPG PAPP Clinical Practice Guidelines For Pediatric Asthma 2021 2Document158 pagesCPG PAPP Clinical Practice Guidelines For Pediatric Asthma 2021 2Kabir SiddiquiNo ratings yet
- TB CPG (PPS)Document28 pagesTB CPG (PPS)Chandice CuaNo ratings yet
- Bronchial Asthma: West Visayas State University Medical Center - Department of PediatricsDocument9 pagesBronchial Asthma: West Visayas State University Medical Center - Department of PediatricsPGI Miayo, StephenNo ratings yet
- PCAP Report ClerkshipDocument54 pagesPCAP Report ClerkshipMichelleAquinoSuzukiNo ratings yet
- Febrile SeizuresDocument5 pagesFebrile SeizuresJulmajir Salipmugdar100% (1)
- PPS Orals List of Topics Case StudiesDocument3 pagesPPS Orals List of Topics Case StudiesEdna M. AtanganNo ratings yet
- Clinical Practice Guideline on Approach and Treatment of Urinary Tract Infection in ChildrenDocument8 pagesClinical Practice Guideline on Approach and Treatment of Urinary Tract Infection in ChildrenPaula QuiñonesNo ratings yet
- Pediatric Tickler by RemDocument7 pagesPediatric Tickler by RemRem AlfelorNo ratings yet
- Managing Acute Infectious Diarrhea in Children CPGDocument10 pagesManaging Acute Infectious Diarrhea in Children CPGKristine Jade OdtujanNo ratings yet
- Philippines TB CP Guidelines 2006Document151 pagesPhilippines TB CP Guidelines 2006wiltechworksNo ratings yet
- Pedia Codigo 2013Document24 pagesPedia Codigo 2013Denise CastroNo ratings yet
- Chronic Suppurative Otitis Media in AdultsDocument10 pagesChronic Suppurative Otitis Media in AdultsRstadam TagalogNo ratings yet
- Hap VapDocument18 pagesHap VapAgita GintingNo ratings yet
- Family Medicine COPCDocument20 pagesFamily Medicine COPCrachellesliedeleonNo ratings yet
- PM PFC MatrixDocument4 pagesPM PFC MatrixFamed residentsNo ratings yet
- Case 1Document12 pagesCase 1Sunny Mae Tura PuigNo ratings yet
- Common Cases in Ambulatory Care Clinic For Lu6Document106 pagesCommon Cases in Ambulatory Care Clinic For Lu6Joy SantosNo ratings yet
- PEDIATRICS Revalida Quick ReviewerDocument2 pagesPEDIATRICS Revalida Quick ReviewerGraziella AndayaNo ratings yet
- Postpartum and Post-op Order GuideDocument7 pagesPostpartum and Post-op Order GuideDre ValdezNo ratings yet
- Medicine OB History and PE TemplateDocument9 pagesMedicine OB History and PE TemplateJanella SuerteNo ratings yet
- 2017 Wise 3RD Year With KeyDocument24 pages2017 Wise 3RD Year With KeyAnne Lorraine BringasNo ratings yet
- Family Life CycleDocument34 pagesFamily Life CycleKathrina AbastarNo ratings yet
- Pediatrics 2 LaboratoryDocument40 pagesPediatrics 2 LaboratoryAmaetenNo ratings yet
- CPG Childhood ImmunizationDocument25 pagesCPG Childhood ImmunizationLady Nur StarkNo ratings yet
- The Hydrocephalus Foundation of The Philippines, Inc.: Save A Life, I PledgeDocument4 pagesThe Hydrocephalus Foundation of The Philippines, Inc.: Save A Life, I PledgejomitraNo ratings yet
- Case 3Document13 pagesCase 3bekbekk cabahugNo ratings yet
- Child PoliciesDocument4 pagesChild PoliciesMon DeNo ratings yet
- PFC MatrixDocument48 pagesPFC Matrixjemma chayocasNo ratings yet
- The "Most Common" . According To NelsonDocument31 pagesThe "Most Common" . According To NelsonKenneth NuñezNo ratings yet
- ROO M General Data Admitt Ing DX Worki NG DX Laboratory Frichmond MedicationsDocument2 pagesROO M General Data Admitt Ing DX Worki NG DX Laboratory Frichmond MedicationsnicewanNo ratings yet
- Pedia - DengueDocument10 pagesPedia - DengueJan Mikhail FrascoNo ratings yet
- Physician's Notes and OrdersDocument2 pagesPhysician's Notes and OrdersEunick VillagraciaNo ratings yet
- Mock Exam 5 23 21Document4 pagesMock Exam 5 23 21Anne Lorraine BringasNo ratings yet
- PAPP Clinical Practice Guidelines For Pediatric Asthma 2021 (Abridged Version)Document69 pagesPAPP Clinical Practice Guidelines For Pediatric Asthma 2021 (Abridged Version)Kai Chua100% (1)
- CPG of Leptospirosis Final VersionDocument128 pagesCPG of Leptospirosis Final VersionxtineNo ratings yet
- Philippine Clinical Practice Guidelines For Acute Otitis Media 2016 LectureDocument53 pagesPhilippine Clinical Practice Guidelines For Acute Otitis Media 2016 LecturePrincess Noreen SavellanoNo ratings yet
- Policy Statements of The Philippine Pediatric Society, IncDocument42 pagesPolicy Statements of The Philippine Pediatric Society, IncMarjorie CepeNo ratings yet
- Clincal Practice Guidelines For Diabetes in The PhilippinesDocument40 pagesClincal Practice Guidelines For Diabetes in The PhilippinesRans NosceNo ratings yet
- 2016.07.18 Pediatrics PREVENTIVE PEDIATRIC HEALTH CARE PDFDocument115 pages2016.07.18 Pediatrics PREVENTIVE PEDIATRIC HEALTH CARE PDFRjDNo ratings yet
- CPG On Acute GastroenteritisDocument24 pagesCPG On Acute GastroenteritisAbegail Fermanejo-Generao100% (1)
- GynexDocument73 pagesGynexDominque RabastoNo ratings yet
- Revalida Reviewer AsmphDocument237 pagesRevalida Reviewer AsmphShey ShocNo ratings yet
- Hester PediatricEthicsFinalProofsDocument9 pagesHester PediatricEthicsFinalProofsFitria FitriaNo ratings yet
- New Intern Guide Quick NotesDocument8 pagesNew Intern Guide Quick NotesTrisNo ratings yet
- Reviewer For Pedia Osce: 10.5 KG 45.16 CM / 17.8 in 75 CM SixDocument10 pagesReviewer For Pedia Osce: 10.5 KG 45.16 CM / 17.8 in 75 CM SixJamora ManilynNo ratings yet
- PPS Policy Statement - Drowning PreventionDocument4 pagesPPS Policy Statement - Drowning PreventionJowairiah RangirisNo ratings yet
- IM AdconDocument28 pagesIM AdconCla SantosNo ratings yet
- Bacterial Men CPGDocument42 pagesBacterial Men CPGKarl Jimenez SeparaNo ratings yet
- Most Common Nelsons 16th EdDocument32 pagesMost Common Nelsons 16th EdRegine PanaliganNo ratings yet
- Fluid and electrolyte management guidelinesDocument12 pagesFluid and electrolyte management guidelinesDavid JonesNo ratings yet
- Copc LectureDocument36 pagesCopc LectureRoger Jr BrazilNo ratings yet
- Philippine Pediatric Society in Cooperation With The Society of Pediatric Critical Care Medicine, PhilippinesDocument32 pagesPhilippine Pediatric Society in Cooperation With The Society of Pediatric Critical Care Medicine, PhilippinesShari TernolaNo ratings yet
- Pathophysiology of Dengue Virus InfectionDocument21 pagesPathophysiology of Dengue Virus InfectionorangepatieNo ratings yet
- List of APMCI Affiliated Hospitals by RegionDocument6 pagesList of APMCI Affiliated Hospitals by RegionJoy ManzanoNo ratings yet
- MINDANAO STATE UNIVERSITY GRAND ROUNDS PROTOCOLDocument14 pagesMINDANAO STATE UNIVERSITY GRAND ROUNDS PROTOCOLArjay Amba0% (1)
- CPG Pcap 2012 PDFDocument54 pagesCPG Pcap 2012 PDFroshmae67% (3)
- Essentials for Practice of Medicine in the Frontline: From Tropical Africa; Pleasantly Different Volume 2From EverandEssentials for Practice of Medicine in the Frontline: From Tropical Africa; Pleasantly Different Volume 2No ratings yet
- CPG Uti PDFDocument7 pagesCPG Uti PDFhellokathyyyyyyNo ratings yet
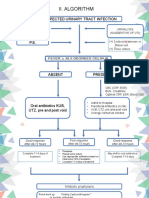
- Ii. Algorithm: Suspected Urinary Tract Infection HistoryDocument6 pagesIi. Algorithm: Suspected Urinary Tract Infection HistoryTaeyomiNo ratings yet
- GINA 2019 Main Report June 2019 Wms PDFDocument201 pagesGINA 2019 Main Report June 2019 Wms PDFAndrada PredaNo ratings yet
- Surgery March 2019Document201 pagesSurgery March 2019hellokathyyyyyy100% (1)
- CPG Uti PDFDocument7 pagesCPG Uti PDFhellokathyyyyyyNo ratings yet
- CPG UtiDocument7 pagesCPG UtihellokathyyyyyyNo ratings yet
- CamScanner Document ScansDocument84 pagesCamScanner Document ScanshellokathyyyyyyNo ratings yet
- AnaPLEDocument20 pagesAnaPLEMc EstanislaoNo ratings yet
- FPCC1Overseas Placements For Sri Lankan Doctors (1) - 2Document3 pagesFPCC1Overseas Placements For Sri Lankan Doctors (1) - 2Thusith WijayawardenaNo ratings yet
- Abnormal Uterine ActionDocument27 pagesAbnormal Uterine ActionSameer KumarNo ratings yet
- Father of Surgery Ayurveda Kashiraj Divodas DhanvantariDocument12 pagesFather of Surgery Ayurveda Kashiraj Divodas DhanvantariDhruv VaghasiyaNo ratings yet
- Jennifer Edson Resume ShortDocument2 pagesJennifer Edson Resume Shortapi-211396777No ratings yet
- Abnormal Expulsive Forces of The UterusDocument2 pagesAbnormal Expulsive Forces of The UterusSayyeda niha AkhtarNo ratings yet
- Dialysis in ChildrenDocument15 pagesDialysis in ChildrenMani VachaganNo ratings yet
- History TPHDocument4 pagesHistory TPHrio80% (1)
- Operating Room Technique Write Up PAPA SLRCDocument43 pagesOperating Room Technique Write Up PAPA SLRCShane Vlademier ParadoNo ratings yet
- Ophthalmic Drops 101Document9 pagesOphthalmic Drops 101David NgNo ratings yet
- 5 PictureDocument1 page5 PictureETC100% (1)
- Bbps4103 - Strategic Management - Assigment 2Document25 pagesBbps4103 - Strategic Management - Assigment 2raj86% (7)
- Application Form Blood Collection Unit Blood StationDocument5 pagesApplication Form Blood Collection Unit Blood StationRhodora BenipayoNo ratings yet
- Bad Obstetric HistoryDocument2 pagesBad Obstetric HistoryRiyan W. PratamaNo ratings yet
- Process of Rapifd PrototypingDocument3 pagesProcess of Rapifd Prototypingpooja rohondiaNo ratings yet
- Dalia Al-Waleed: About MeDocument3 pagesDalia Al-Waleed: About MeAlaa JamoosNo ratings yet
- 00014Document6 pages00014Paulo VictorNo ratings yet
- Project Sahayata - Fighting Cancer - RediffDocument5 pagesProject Sahayata - Fighting Cancer - RediffudayNo ratings yet
- Trigeminal Neuralgia Guide: Causes, Symptoms and Treatment OptionsDocument4 pagesTrigeminal Neuralgia Guide: Causes, Symptoms and Treatment OptionsTiger_2011No ratings yet
- CSF Dynamics in Dandy-Walker Syndrome ExplainedDocument5 pagesCSF Dynamics in Dandy-Walker Syndrome ExplainedSergio SaraivaNo ratings yet
- (Ob) - 4s-1-Antepartum Surveillance and Intrapartum MonitoringDocument8 pages(Ob) - 4s-1-Antepartum Surveillance and Intrapartum MonitoringKim RamosNo ratings yet
- ReferencesDocument2 pagesReferencesDiane-Richie PezLoNo ratings yet
- IhtDocument22 pagesIhtkaliyugaaNo ratings yet
- Canine InsulinomaDocument5 pagesCanine Insulinomasoff4ikaNo ratings yet
- The Center For Endometriosis Care Welcomes Dr. Jeffrey T. Arrington To The CEC TeamDocument3 pagesThe Center For Endometriosis Care Welcomes Dr. Jeffrey T. Arrington To The CEC TeamPR.comNo ratings yet
- Alsa Excell 200 MCDS - Manual de ServicioDocument17 pagesAlsa Excell 200 MCDS - Manual de ServicioAlberto0% (1)
- Concept and History of Nursing EducationDocument5 pagesConcept and History of Nursing Educationmazumderr179No ratings yet
- Central Venous Pressure MonitoringDocument2 pagesCentral Venous Pressure MonitoringpauchanmnlNo ratings yet
- Test 1 English For NursingDocument2 pagesTest 1 English For NursingJuanARNo ratings yet
- Fracture of PatellaDocument22 pagesFracture of Patellaabdul azizNo ratings yet