Placental Gas Exchange and the Oxygen Supply
to the Fetus
Anthony M. Carter*1
ABSTRACT
The oxygen supply of the fetus depends on the blood oxygen content and flow rate in the uterine
and umbilical arteries and the diffusing capacity of the placenta. Oxygen consumption by the
placenta is a significant factor and a potential limitation on availability to the fetus. The relevance
of these several factors as well as responses to acute or sustained hypoxia has been explored
in the sheep model. In addition, much has been learned in the context of hypobaric hypoxia
by studying human populations that have resided at high altitude for varying periods of time.
Embryonic development occurs under anaerobic conditions and even the fetus is adapted to a
low oxygen environment. Nevertheless, there is a reserve capacity, and during acute hypoxia the
fetus can counter a 50% reduction in oxygen delivery by increasing fractional extraction. During
sustained hypoxia, on the other hand, fetal growth is slowed, although oxygen consumption is
unaltered when corrected for fetal mass. Similarly, birth weight is reduced in humans living at
high altitude even if the effect is tempered in those with a long highland ancestry. Placental mass
changes little during sustained hypoxia in sheep or humans at high altitude. This conceals the fact
that there are structural changes and that placental oxygen consumption is reduced. The underlying
mechanisms are a current focus of research. One intriguing possibility is that increased anaerobic
metabolism of glucose in the placenta spares oxygen for the fetus but reduces its supply of substrate
and thereby limits fetal growth. © 2015 American Physiological Society. Compr Physiol 5:1381-
1403, 2015.
Introduction In contrast, human pregnancy at high altitude offers an
interesting natural experiment in chronic maternal hypoxia.
An acute reduction in fetal oxygen supply can have serious Although the first observations date back 60 years (114),
consequences. Monitoring of fetal heart rate and oxygen status research on high-altitude hypoxia continues to offer new
during delivery is therefore standard clinical practice. The aim insights. It represents our second major source of informa-
is to reduce the incidence of perinatal death and of patholo- tion and here is treated accordingly. Populations that have
gies such as cerebral palsy. Chronic hypoxia, where the oxy- been resident in the highlands for many generations (e.g.,
gen supply is limited over time, may result in fetal growth Andeans and Tibetans) have fewer pregnancy complications
restriction with long-term consequences for health, includ- and higher birth weights than recent immigrants (e.g., Euro-
ing a higher incidence of cardiovascular disease in adult life. peans and Han). Comparison of these groups continues to
Because placental gas exchange and fetal oxygen supply play improve our understanding of the role of the placenta in fetal
critical roles for obstetric and pediatric outcomes, a wealth oxygenation. As an example, the ability of the placenta to
of experimental data has accumulated about the factors that downregulate its own oxygen consumption in favor of the
determine them. fetal oxygen supply is now better understood because of
A major source of information stems from experiments work on high-altitude placentas. Additionally, this body of
in sheep, where sophisticated techniques have been devel- work supports the assumption that the physiology of placen-
oped to study the ewe and her fetus. The heyday for such tal gas exchange is similar in ovine and human pregnancies
research was 25 to 40 years ago and there are several com- at term.
prehensive reviews (35, 125, 218). It is commonly assumed
that the sheep data can be translated to human pregnancy. As
an example, textbooks of physiology often give values for
oxygen saturation in the fetal circulation without acknowl- * Correspondence to acarter@health.sdu.dk
edging that the data derive from sheep. However, clinical 1 Cardiovascular and Renal Research, Institute of Molecular Medicine,
correlates can be hard to find. Although uterine and umbilical University of Southern Denmark, Odense, Denmark
blood flows can be estimated noninvasively by Doppler ultra- Published online, July 2015 (comprehensivephysiology.com)
sound, it is difficult to pair them with values for blood oxygen DOI: 10.1002/cphy.c140073
content. Copyright © American Physiological Society.
Volume 5, July 2015 1381
Placental Gas Exchange Comprehensive Physiology
Some Basic Concepts and Animal Models Table 1 Values Pertinent to Arterial Oxygen Transport in the Term
Fetus, Male High-Altitude Climbers at 8400 m on Mount Everest and a
Typical Adult Male
The oxygen environment of the fetus
In the first trimester of human pregnancy, the fetus and pla- Climbers at
centa need to be protected from exposure to high oxygen Term fetus 8400 m Adult male
levels. The danger to the developing embryo stems from the
threat posed by reactive oxygen species (ROS) such as the PaO2 , (kPa (mmHg)) 2.5-3.5 (19-26) 3.28 (25) 13.3 (100)
superoxide (O. 2 − ) and hydroxyl (OH. ) anions and their non-
SaO2 (%) 65 54 98
radical intermediates such as hydrogen peroxide (33). Conse-
PaCO2 , (kPa (mmHg)) 5.3-6.6 (40-50) 1.77 (13) 4.7-6.0 (35-45)
quently, the supply of maternal blood to the intervillous space
is sluggish or even absent during the first 10 weeks of ges- pH 7.25-7.35 7.53 7.35-7.45
tation (90). On the fetal side, embryonic hemoglobins with Hb (g dL−1 ) 16.6 19.3 15.0
high oxygen affinity (29, 108) act to sequester oxygen rather P50 , (kPa (mmHg)) 2.5 (19) 3.6 (27) 3.5 (26)
than transport it to the tissues.
CaO2 , (mL L−1 ) 150 145 200
The low oxygen levels endured by the early embryo make
sense when viewed in an evolutionary perspective. The atmo- Reproduced from (138) © 2010 Biomed Central Ltd.
sphere and the oceans were devoid of oxygen during most
of earth’s history. This changed during the Great Oxidation
Event 2.4 to 2.0 billion years ago, but for long after the oxy- Oxygen delivery to the fetus (mmol min−1 ) is given by the
gen content of the atmosphere was a fraction of present day product of umbilical blood flow (mL min−1 ) and the oxygen
levels (73, 179). Although atmospheric oxygen rose intermit- content ([O2 ]) of umbilical venous blood (mmol L−1 ):
tently 850 to 540 million years ago, oxygenation of the oceans
remained low in the Cryogenian Period when the first traces of Fetal O2 delivery = Umbilical blood flow × [O2 ]umbilical vein
sponges appear (134). Interestingly, present day sponges can (1)
maintain respiration, feeding, and growth at equivalent levels
of oxygenation (0.5%-4.0% of present atmospheric levels) Oxygen uptake by the fetus is the product of umbilical
(149). Returning to the first trimester human fetus, it thrives blood flow and the difference in oxygen content across the
in a low oxygen environment by relying on the phylogenet- fetal placental circulation:
ically ancient polyol pathway. That enables it to metabolize
glucose and regenerate NAD+ and NADP+ under anaerobic Fetal O2 uptake = Umbilical blood flow
conditions without producing lactate. This was confirmed by
× ([O2 ]umbilical vein − [O2 ]umbilical artery ) (2)
analysis of amniotic and celomic fluid from the first trimester
human fetus (89), but the pathway may be maintained by the
placenta later in gestation as indicated by the transplacental The values obtained in Eqs. (1) and (2) frequently are
gradients for polyols in sheep (201). Blood flow through the corrected for fetal mass and given in mmol min−1 kg−1 . In
intervillous space starts to rise around 12 to 14 weeks and steady state, fetal oxygen uptake is equal to fetal oxygen
this change is accompanied by increased expression in the consumption.
placenta of ROS scavengers such as superoxide dismutase Fetal oxygen extraction is the ratio of oxygen uptake to
(90, 212). oxygen delivery and often is expressed as a percentage:
Even after the increase in maternal placental blood flow,
PO2 in the umbilical vein (the most highly oxygenated fetal Fetal O2 extraction = Fetal O2 uptake∕Fetal O2 delivery × 100
blood) is as low as 30 mmHg (4.0 kPa) with an oxygen satu- (3)
ration of around 85% (218). Despite the physiological shunts
offered by the ductus venosus and foramen ovale, blood reach- Oxygen delivery to the gravid uterus is given by:
ing the heart and brain has a PO2 of 25 mmHg (3.3 kPa) and
a saturation of at most 65%. Thus what might be considered Uterine O2 delivery = Uterine blood flow × [O2 ]uterine artery
hypoxia in postnatal life is normoxia to the fetus. This led (4)
Sir Joseph Barcroft to coin the concept of “Everest in utero”
(138, 220) (Table 1). Uterine oxygen uptake is obtained by:
Oxygen delivery, oxygen uptake, and oxygen Uterine O2 uptake = Uterine blood flow
extraction × ([O2 ]uterine artery − [O2 ]uterine vein ) (5)
It is important to distinguish between fetal oxygen delivery
and uptake, on the one hand, and oxygen delivery to the Analogous with Eq. (3), uterine oxygen extraction is the
uteroplacental unit (including the fetus), on the other. ratio of oxygen uptake to oxygen delivery.
1382 Volume 5, July 2015
Comprehensive Physiology Placental Gas Exchange
The difference between uterine and fetal oxygen uptake A minor drawback of the sheep as a model is the occur-
gives oxygen uptake by the placenta and uterine wall: rence of two types of hemoglobin with different affinities for
oxygen. Thus the P50 of maternal blood depends on whether
Placental O2 uptake = Uterine O2 uptake − Fetal O2 uptake the ewe is homozygous for type A hemoglobin (P50 = 31.3
(6) mmHg), homozygous for type B (P50 = 40.7 mmHg), or
heterozygous (AB; P50 = 35.7 mmHg) (135). A careful com-
Some studies use Eq. (6) to calculate placental oxygen parison of pregnant ewes that were either AA or BB found
uptake and do not distinguish between oxygen usage by the that the difference in maternal blood oxygen affinity was com-
placenta and uterine wall. This is an approximation given that pensated to the extent that their fetuses had similar levels of
about 15% of uterine blood flow supplies the endometrium oxygenation (219).
and myometrium (137). Data obtained in sheep have been used for mathematical
modeling of placental gas exchange. This is a useful approach
that allows predictions to be made about the impact of altering
Animal models a single variable or set of variables. The principles of placental
Some of the variables in the above equations can be deter- modeling are embodied in the work of Hill, Power, and Longo
mined acutely at Cesarean section, but the oxygen content of (71, 130) and are reviewed elsewhere (125).
uterine venous blood cannot and some would dispute whether One advantage of the sheep is its size and the fact that like
maternal placental or uterine blood flow can be measured humans it gives birth to a highly developed neonate. Placen-
accurately by current imaging techniques (198). Certainly, tation in the sheep is, however, different in several respects
there is no scenario where these variables can be altered from human placentation (Table 3). While a human placenta
to examine the acute and chronic responses of the system. is discoid with an intervillous space and a hemochorial pla-
Therefore, much of our knowledge of placental gas trans- cental barrier, the ovine placenta is cotyledonary, lacks an
fer is based on experimental work in sheep. The model was intervillous space, and has an epitheliochorial barrier (43).
pioneered by Sir Joseph Barcroft, Donald H. Barron, and There are more layers of tissue in an epitheliochorial than a
Geoffrey Dawes [reviewed by (126)]. An important break- hemochorial placenta. However, several adaptations result in
through came in the 1970s when techniques were developed a diffusion distance from maternal to fetal blood that is not
for the chronic catheterization of the umbilical and uterine much greater in ovine than in human placenta. Techniques
blood vessels (142). This enabled studies to be made in the have been developed for the baboon (59,96,199), which has a
unstressed ewe and her fetus without the confounding effects placenta similar to our own (Table 3), and although the body
of anesthesia and surgical stress (12). Representative values of data is much smaller, it suffices to support the assertion
for the principal factors affecting placental oxygen transfer in that the sheep is an adequate model to study placental gas
midgestation and late gestation sheep are given in Table 2. To exchange (38).
model high-altitude pregnancy, the techniques developed in Placentation in rodents differs in several respects from
sheep have been adapted for studies in unstressed llamas and human placentation (Table 3). The chorioallantoic placenta
their fetuses, the llama being an inhabitant of the altiplano is labyrinthine rather than villous and there is an additional
(21, 120, 121). yolk sac placenta that functions throughout gestation. The
Table 2 Reference Values for the Principal Factors Affecting Placental Oxygen Transfer in the Ewe and Fetal Sheep in
Midgestation (71-81 days) (19) and Late Gestation (133 ± 1 days) (219)
Variable Midgestation Late gestation
Uterine blood flow (mL min−1 ) 657 ± 77 1132 ± 83
Maternal hemoglobin concentration (mmol L−1 ) 7.3 ± 0.3 6.6 ± 0.2
Maternal arterial oxygen saturation (%) 92.8 ± 0.6 89.4 ± 0.6
Umbilical blood flow (mL min−1 ) 100 ± 12 571 ± 40
Umbilical blood flow (mL min−1 kg−1 fetus) 468 ± 57 189 ± 10
Fetal hemoglobin concentration (mmol L−1 ) 5.7 ± 0.3 7.1 ± 0.3
Umbilical venous oxygen saturation (%) 89.6 ± 1.1 79.7 ± 2.0
Fetal oxygen uptake (mmol min−1 ) 0.11 ± 0.01 1.02 ± 0.09
Fetal oxygen uptake (mmol min−1 kg−1 fetus) 0.486 ± 0.027 0.329 ± 0.006
Oxygen uptake by myoendometrium and placenta (mmol min−1 ) 0.57 ± 0.07 0.63 ± 0.06
All values are mean ± SEM.
Volume 5, July 2015 1383
Placental Gas Exchange Comprehensive Physiology
Table 3 Comparison of Placentation in the Human and Some Common Animal Models
Baboon and rhesus
Human macaque Mouse Guinea pig Sheep and llama
Implantation Primary interstitial Superficial Secondarily Secondarily interstitial Superficial
interstitial
Decidualization Spontaneous Spontaneous Induced Induced Absent
Placental shape Discoid Discoid Discoid Discoid Cotyledonary
Internal structure Intervillous space Intervillous space Labyrinthine Labyrinthine Interdigitating villi
Interhemal barrier at Hemomono-chorial Hemomonochorial Hemotrichorial Hemomonochorial Epitheliochorial
term
Trophoblast invasion Interstitial and Interstitial to decidua Interstitial to decidua Interstitial and Absent
endovascular to inner endovascular at least to
third of myometrium myometrium
Yolk sac Never forms a Never forms a placenta Permanent inverted Permanent inverted yolk Temporary yolk sac
placenta yolk sac placenta sac placenta placenta
Gestation length 268 days 160 days 19 days 64 days Sheep 148 days;
llama about 350
days
Litter size Usually one Usually one 4-12 About 4 1-2
Neonate Precocial Precocial Altricial Precocial Precocial
mouse and most other murine rodents have short gestations Embolization of the umbilical circulation by repeated
and poorly developed (altricial) neonates. Placental oxygen injection of microspheres targets umbilical blood flow and
transfer may be critical only in the last few days making fetal oxygen delivery (61). This model has been used mainly
them less satisfactory as models of fetal oxygenation (38,44). to explore fetal endocrine responses to hypoxia (40, 62) and
In addition, most of the relevant variables are difficult to remodeling of fetal blood vessels (204).
measure in these species, although progress has been made
in measuring flow velocities in the uterine, umbilical, and
vitelline arteries of the mouse (163). Guinea pigs have a longer
gestation and deliver mature (precocial) young. Some work Vascular Architecture and Placental
has been done on placental oxygen transfer in this species Blood Flows
although mainly in acute experiments and under anesthesia
(36). Labyrinthine and villous placentas
In many mammals, the exchange area of the placenta is a
labyrinth in which fetal and maternal capillaries (maternal
Modeling fetal growth restriction in sheep
blood channels in hemochorial placentas) run parallel to one
Currently there is a strong focus on fetal growth restriction and another. The direction of blood flow is opposite in the fetal
its implications for future health (64). The placenta is increas- and maternal circuits, allowing for countercurrent exchange
ingly seen to play a key role in what is generally defined as (147). This is an efficient system when exchange is flow-
developmental programming (34, 113). Much of the relevant dependent as is the case for oxygen. Interestingly, neither the
research concerns the nutrient supply to mother and fetus and sheep nor the human placenta conforms to the countercurrent
is beyond the scope of this overview. pattern. Concurrent flow is assumed in mathematical models
There are, however, animal models of fetal growth restric- of the ovine placenta (125). However, recent work employ-
tion that target variables important for placental gas exchange. ing microvascular corrosion casting and scanning electron
One of these, developed by Alexander (4), relies on the microscopy has shown there is a mix of concurrent, cross-
fact that the ovine placenta is made up of numerous placen- current, and countercurrent flow in the sheep placenta (66). In
tomes (approx. 60-100) formed at preexisting structures in the human placenta, the fetal capillaries are found at the tips of
endometrium called caruncles. The number of placentomes the villous trees whilst maternal blood flows through the inter-
formed can be reduced by excising most of the caruncles villous space. This is best approximated as crosscurrent flow,
prior to pregnancy. This procedure, known as carunclectomy, although clearly there will be concurrent and countercurrent
affects uterine and umbilical blood flows and oxygen delivery components, a pattern sometimes referred to as “multivillous
to the gravid uterus and fetus (167, 168). flow.”
1384 Volume 5, July 2015
Comprehensive Physiology Placental Gas Exchange
Does this entail that oxygen transfer is less efficient in It seems unlikely, therefore, that fetal oxygenation is much
the human placenta than that of the mouse or guinea pig? A affected by the reductions in uterine blood flow that occur
stringent analysis by Metcalfe et al. (144) showed the advan- during uterine contractions. This view is supported by a study
tage of countercurrent over “multivillous” flow is not as great where uterine oxygen uptake was measured during uterine
as sometimes thought. In the human placenta, it likely is over- contraction on a moment-to-moment basis (128). The system-
ridden by the greater volume flow that can be achieved in the atic changes in uterine blood flow and oxygen uptake during
low-resistance intervillous space (39). spontaneous or oxytocin-induced contractions were no greater
than the random variations seen during uterine quiescence.
The ovine fetus can maintain its oxygen consumption dur-
Uterine and placental vasculature ing even a 24-h reduction in uterine blood flow (25, 75). Pro-
Maintenance of an adequate blood flow through the mater- longed reductions of uterine blood flow can, however, impact
nal placental circulation requires far reaching changes in on fetal growth. Thus, when a reduction in uterine blood flow
the upstream vessels, especially the uterine arteries and their was maintained for 7 days, by partial occlusion of the aorta,
branches. Responses to pregnancy include increases in vessel the linear growth rate of the fetus decreased by 38% over
diameter, remodeling of the vessel wall and changes in vasore- controls and growth rate was correlated to oxygen delivery
activity [reviewed by (206)]. One current focus of research (27). Interestingly, fetal uptake of glucose and oxygen was
is the role played by potassium channels in uterine vascu- sustained, despite a sizeable decrease in oxygen delivery. Pla-
lar adaptation to pregnancy, including the response to sex cental mass was 20% smaller in occluded animals compared
hormones (226). We are also gaining information about the to controls and this was interpreted as an adaptive response
importance of intercellular communication through gap junc- (27). In a more recent study (111, 112), uterine blood flow
tions as it pertains to the regulation of smooth muscle tone by was clamped at 750 mL min−1 from day 113 of gestation to
endothelium-derived factors like nitric oxide and prostacyclin day 138, a week before term. Over the same period uterine
(5). In human pregnancy, there is extensive remodeling of the blood flow in control animals rose to 1409 mL min−1 . The
uterine spiral arteries that supply the intervillous space; both procedure led to asymmetric growth restriction with a 32%
maternal factors and invasive trophoblast are important for reduction in fetal body weight, but no significant decrease in
this process (67, 178). brain weight. There was a 27% decrease in placental weight
(111).
Uterine blood flow
The diameter of the uterine artery and the rate of uterine blood Umbilical blood flow
flow both increase in linear fashion during human pregnancy Reviewing estimates of umbilical blood flow in human preg-
(203). Accurate and reproducible measurements of uterine nancy, Battaglia and Meschia (14) concluded that some stud-
blood flow in pregnant women are, however, difficult to obtain ies were biased by large systematic errors in the calculation of
(14). The oxygen saturation of uterine venous blood at term blood flow. On physiological grounds, they were inclined to
is about 80% (60). With this as a starting point, Battaglia and accept estimates at the high end of the range (about 120 mL
Meschia (14) recently estimated a uterine blood flow of about min−1 kg−1 fetal mass). Umbilical blood flow is increased
800 mL min−1 or 270 mL min−1 kg−1 fetal mass, which is at in term human fetuses as compared to preterm ones (118).
the high end of the range of values obtained by ultrasound. Calculated per unit of fetal mass, however, umbilical blood
Uterine blood flow was reduced in pregnancies with fetal flow is seen to decrease with advancing gestation (118).
growth restriction compared to those where the fetal weight Umbilical blood flow in sheep was seen to vary widely
was appropriate for gestational age (109). The reproducibility without any significant change in fetal oxygen uptake at low
of measurements purporting to reflect blood flow through or high rates of flow (46). When umbilical blood flow was
the intervillous space has been called into question (198). reduced, by occluding the cord for 3 to 4 min, the resultant
Fortunately, there are reliable measurements in sheep under a decrease in oxygen delivery was accompanied by a progres-
range of experimental conditions. sive increase in fetal oxygen extraction (80). Umbilical blood
Oxygen uptake by the ovine fetus was shown to be insensi- flow could be reduced by almost half without influencing fetal
tive to variations in uterine blood flow (217). A 45% reduction oxygen uptake. Indeed, due to the high oxygen affinity of fetal
in fetal oxygen delivery led to a fall in fetal arterial oxygen hemoglobin, the fetus was capable of a remarkable increase
content from 4 to 2 mmol L−1 . But this did not cause any in fractional oxygen extraction, which rose from 34% to 68%
appreciable change in fetal oxygen uptake because of a com- when umbilical blood flow was reduced by 75%. This degree
pensatory increase in fractional oxygen extraction. In contrast, of cord compression was, however, associated with a fall in
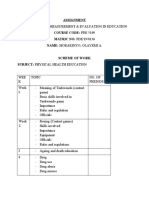
a marked reduction in fetal oxygen uptake occurred when oxy- fetal oxygen uptake (Fig. 1).
gen delivery was decreased by more than 55% (to <0.5 mmol The interval within which fetal oxygen uptake was main-
min−1 kg−1 ). Thus, under normal physiological conditions, tained could be extended by allowing the ewe to breathe 100%
the oxygen supply to the fetal lamb is approximately twice oxygen rather than room air (57). During this treatment, oxy-
that needed to maintain an adequate fetal oxygen uptake. gen delivery improved because of a 15% to 20% rise in the
Volume 5, July 2015 1385
Placental Gas Exchange Comprehensive Physiology
14 1 blood flow (6). There did not appear to be a threshold level for
y = –276.80 X
+ 8.49
umbilical blood flow above which fetal oxygen uptake was
r = 0.84
O2 consumption (mL min–1 kg–1)
P < 0.001 maintained at control levels. This may partly explain why
fetal growth fell from 4% per day to 2% per day when reduc-
10 tions in umbilical blood flow were maintained for several days
or weeks (6). Commenting on the subtle difference between
the results of short-term and long-term reduction of umbilical
blood flow, Anderson et al. (8) suggested that fetal oxygen
6 consumption can be turned down only slowly in response to
a reduced oxygen supply.
2 Mismatching of maternal and fetal placental blood
–75% –50% –25% C flows
Mathematical modeling indicates that placental gas exchange
40 120 200 280
will be most efficient when fetal and maternal blood flows are
Umbilical blood flow (mL min–1 kg–1)
perfectly matched. This has been looked at in sheep by inject-
ing radionuclide-labeled microspheres into both circulations
and measuring their distribution in small samples of placenta
80 (cubes about 2-3 mm on edge). The maternal:fetal blood flow
y = –58.18 log X + 173.44 ratio was <0.5 in 9% of the samples, 0.5 to 1.5 in 70% and
r = –0.91 >1.5 in the remaining 21%. When these numbers were fed
P < 0.001 into a mathematical model of placental gas exchange, it was
O2 extraction (%)
60 found that mismatching of flows reduced the predicted PO2
of umbilical venous blood by ca. 6 mmHg (181).
40
Blood Oxygen Capacity and Affinity
Embryonic and fetal hemoglobins
20 Hemoglobin is a heterotetramer comprised of two alpha and
–75% –50% –25% C two beta globin chains each with an associated heme group.
There are multiple isoforms of the alpha and beta chains
40 120 200 280 encoded by separate cassettes of genes located on differ-
Umbilical blood flow (mL min–1 kg–1) ent chromosomes. Importantly, gene expression is develop-
Figure 1 Effect on fetal oxygen consumption (upper panel) and oxy-
mentally regulated, resulting in embryonic, fetal, and adult
gen extraction (lower panel) of reducing umbilical blood flow in the hemoglobins. The principal hemoglobins expressed during
fetal lamb by partial cord occlusion. Error bars are SD. Reproduced, human development are listed in Table 4. The nomenclature
with permission, from (80); Copyright © 1983 with permission from used for the globin genes is that proposed by Aguileta et al.
Elsevier.
(2) with traditional nomenclature given in parentheses.
Gower I expression begins coincident with the production
oxygen content of umbilical venous blood and fetal oxygen of nucleated red cells in the yolk sac. This hemoglobin has a
uptake was maintained over a significantly wider range of P50 of 4 mmHg and a very low sensitivity toward modulation
umbilical blood flows than in experiments where the ewe of oxygen affinity, properties reminiscent of myoglobin (29).
breathed room air. A second study confirmed the beneficial Its function may be to sequester oxygen rather than transport
effect of 100% oxygen, although noting it was less effective at it to the tissues. This could also be the case with Portland
severe degrees of blood flow reduction (172). Together these I, the intermediate embryonic hemoglobin. Gower II, on the
studies suggest that there is a wide margin of safety in pla- other hand, has a somewhat lower oxygen affinity (72) (Fig. 2)
cental oxygen transfer during acute reductions in umbilical and shares properties with fetal hemoglobin (29). The oxygen
blood flow lasting a few minutes, which may be of clinical affinity of embryonic hemoglobin in other species is likely to
relevance in the context of cord compression in labor. be high based on findings in the mouse (17), rabbit (74, 91),
A rather different picture emerged during long-term and pig (214).
reduction of fetal placental blood flow, achieved by inflat- The high oxygen-binding affinity of fetal blood facilitates
ing an occluder around the distal aorta. In experiments where placental oxygen transfer (Fig. 3). If, for example, maternal
computer-controlled restriction of flow was maintained for and fetal bloods equilibrate at a PO2 of 30 mmHg, the mater-
10 days, fetal oxygen uptake was linearly related to umbilical nal hemoglobin will be about 50% saturated whilst the fetal
1386 Volume 5, July 2015
Comprehensive Physiology Placental Gas Exchange
Table 4 Human Embryonic, Fetal, and Adult Hemoglobins
Hemoglobin Ontogeny Alpha chain Beta chain P50 (mmHg)
Gower I Embryonic (predominant days 15-37) HBZ-T1 (ζ) HBE (ε) 4
Portland I Embryonic (from 4 weeks) HBZ-T1 (ζ) HBG-T1 (γ1 ) 6
Gower II Embryonic (from 4 weeks) HBA-T1, HBA-T2 (α2 , α1 ) HBE (ε) 12
Fetal (HbF) Fetal and early postnatal HBA-T1, HBA-T2 (α2 , α1 ) HBG-T1, HBG-T2 (γ1 , γ2 ) 20
Adult (HbA) Late fetal and adult HBA-T1, HBA-T2 (α2 , α1 ) HBB (β) 26
Adult (HbA2 ) Adult (3%) HBA-T1, HBA-T2 (α2 , α1 ) HBD (δ) 26
hemoglobin will have achieved an oxygen saturation of about by developmental regulation of two enzymes associated with
80%. DPG metabolism (92).
However, whilst all mammals have embryonic
hemoglobins (108), not all have a fetal hemoglobin. Human Oxygen affinity of fetal blood
fetal hemoglobin is the result of a gene duplication that
The oxygen affinity of hemoglobin is inversely proportional
occurred in the lineage of anthropoid primates (182). The
to the concentration of its three other ligands: hydrogen
sequence in which beta globin genes are expressed is a func-
ion, carbon dioxide, and DPG. Human hemoglobin F has a
tion of their distance from a common locus control region.
lower affinity for DPG than hemoglobin A and a correspond-
Tandem gene duplication resulted in a copy of an embryonic
ingly higher affinity for oxygen (16). During placental gas
gene that was further from the locus control region and came
exchange, the PCO2 of maternal blood rises, and the pH falls,
to be expressed later in development (95). In an interesting
which diminishes the oxygen affinity of maternal hemoglobin
example of convergence, a fetal hemoglobin was evolved in
(the Bohr Effect). The reverse process occurs in fetal blood,
the bovid family of ruminants, which includes the sheep and
increasing the oxygen affinity of fetal hemoglobin. The dou-
goat. In this instance, it arose by tandem duplication of the
ble Bohr Effect enhances the difference in oxygen affinity
HBB gene (117).
between maternal and fetal blood and it accounts for an esti-
In most other mammals, including murine rodents, fetal
mated 8% of placental oxygen transfer (71, 144).
and maternal blood contain the same type of hemoglobin (32).
To evaluate the importance of the difference in oxygen
Fetal blood nevertheless has a higher oxygen affinity due to
affinity, Itskovitz et al. (79) raised the P50 of fetal blood from
a the low 2,3-diphosphoglycerate (DPG) content of the fetal
20 to 41 mmHg, an oxygen affinity corresponding to that
red cells (39). It has been shown in the rat that this is achieved
of adult sheep hemoglobin, by exchange transfusion of the
fetus with maternal blood. Secondary to the reduced oxygen
affinity, there was a fall in the oxygen saturation of umbil-
100 ical venous blood, resulting in a decrease in oxygen con-
tent from ca. 4 to 2 mmol L−1 . Umbilical blood flow also
80 decreased following the exchange transfusion, and oxygen
delivery to the fetus fell by 64%. Fetal oxygen uptake fell
by 44% and metabolic acidosis developed, causing a further
Saturation (%)
60
rightward shift of the oxygen dissociation curve. The right-
ward shift limited the efficiency of oxygen unloading to the
40 fetal tissues and thus the ability of the fetus to compensate
for reduced oxygen delivery by increasing oxygen extraction.
20 Therefore, mean fetal oxygen extraction was only 51% fol-
lowing exchange transfusion with maternal blood (79).
The long-term effects on fetal oxygenation and develop-
0
0 10 20 30 40 50 ment of replacing fetal blood with adult blood are not com-
PO2 (mmHg)
pletely known. Human fetuses given transfusions of adult red
cells to treat hemolytic disease of the fetus and newborn have
Figure 2 Oxygen binding to human embryonic hemoglobins. The survived with normal growth indices and fairly normal acid-
saturation of hemoglobin with oxygen as a function of PO2 is shown for base values at birth (166, 193, 211). The effect of exchange
adult hemoglobin (black circles) and embryonic hemoglobins Gower I transfusion may be less pronounced in humans than in sheep
(black inverted triangles), Portland (open circles), and Gower II (open
squares). Reproduced, with permission, from (29); Copyright © 2002 as the difference between fetal and maternal P50 is smaller
with permission from Elsevier. (79).
Volume 5, July 2015 1387
Placental Gas Exchange Comprehensive Physiology
24
10
22
9
20
8 18 Fetus
16 v
4.6 mL . dL–1
7 A
*
O2 content (mL . dL–1)
O2 content (mmol L–1)
5 mL . dL–1
6 14
Mother
12
5 a
10 *
V
4
8
3
6
2
4
1 2
0 0
0 10 20 30 40 50 60 70 80 90 100
Oxygen tension (mmHg)
Figure 3 Blood oxygen content as a function of PO2 for human maternal and near term fetal blood. A and V,
maternal arterial and venous values; a and v, umbilical arterial and venous values. Reproduced, with permission,
from (125); Copyright © 1987 The American Physiological Society.
Oxygen affinity of maternal blood if an increase in oxygen capacity were achieved at the expense
of a drop in umbilical blood flow.
Maternal hyperventilation in labor causes a fall in PCO2 and
Chronic intrauterine hypoxia stimulates the secretion of
rise in pH of maternal blood and this leads to a reduction in
erythropoietin, resulting in increased red cell production (52).
fetal PO2 (148, 209). In part, the response can be attributed to
In addition to the fetal kidneys, human placenta is a potential
the resultant increase in maternal oxygen affinity, since closer
source of erythropoietin (51, 52). Polycythemia is associated
approximation of the maternal and fetal oxygen dissociation
with fetal growth restriction and may reflect an attempt at
curves entails that equilibrium between the blood of mother
compensation (202). Note, however, that polycythemia may
and fetus is reached at a lower PO2 .
in itself impede growth because the associated increase in
Women with high-affinity blood (hemoglobinopathies)
blood viscosity can have a negative impact on oxygen delivery
have successful pregnancies (157, 170), however, indicating
(200).
that a difference in oxygen affinity between maternal and
The effect of raising or lowering fetal hematocrit has been
fetal blood is not a prerequisite for fetal survival. There is,
evaluated in sheep by isovolemic exchange transfusion with
nonetheless, a higher incidence of perinatal morbidity and
packed red blood cells or plasma from a donor fetus (55). Fetal
small-for-gestational-age babies in mothers with sickle cell
oxygen delivery was maximal at a hematocrit of 33% (Fig. 4).
disease (45, 76).
When fetal hematocrit was increased above the optimal value,
oxygen delivery decreased because the reduction in umbili-
cal blood flow was proportionately greater than the rise in
Oxygen capacity of fetal blood umbilical venous oxygen content. Fetal oxygen uptake was,
The oxygen-carrying capacity of blood is largely a function however, relatively constant at hematocrits between 16% and
of hematocrit, since the intraerythrocytic hemoglobin con- 48%, because fractional oxygen extraction increased to com-
centration is rather constant and the contribution of dissolved pensate for the reduction in oxygen delivery. At hematocrits
oxygen is negligible. The hematocrit is higher in fetal than <16% or >48%, corresponding to a fetal oxygen delivery
maternal blood so it is worth noting that hematocrit also is a <0.6 mmol min−1 kg−1 , oxygen uptake by the fetus decreased.
major determinant of blood viscosity and influences the rate This was associated with a fall in base excess, confirming that
of blood flow. Clearly, no advantage would accrue to the fetus oxygen delivery to some fetal tissues was inadequate to meet
1388 Volume 5, July 2015
Comprehensive Physiology Placental Gas Exchange
40 isovolemic exchange transfusion with plasma or packed red
cells from pregnant donor sheep (initial hematocrit 27%).
DO2 fetus (mL O2 min–1 kg–1)
y = –19.7 + 2.59x – 0.039x2 Uterine blood flow did not alter and oxygen delivery to the
30
uterus decreased linearly with decreasing hematocrit. Oxygen
consumption by the uterus, placenta, and fetus decreased only
20 slightly, however, because of increased oxygen extraction. On
the fetal side, both umbilical venous oxygen content and oxy-
10 gen delivery to the fetus fell with decreasing maternal hema-
tocrit. But even when fetal oxygen delivery was reduced by
50%, oxygen uptake was kept constant by a compensatory
0 increase in fetal oxygen extraction. When maternal hemat-
100 ocrit and fetal oxygen delivery were decreased by more than
y = 124 – 5.9x + 0.09x2 50%, fetal oxygen uptake fell, because the increased extrac-
80 tion did not fully compensate for the additional reduction in
fetal oxygen delivery. An oxygen delivery of >6 mmol min−1
Fetal O2 extraction (%)
kg−1 was required to maintain oxidative metabolism. At lower
60 rates there was a decrease in the base excess of fetal arterial
blood.
40 When maternal anemia (hematocrit 14%) was maintained
for 6 days, there was a compensatory increase of 35% in utero-
placental blood flow. There was still a net reduction in oxygen
20
delivery to the gravid uterus, but its oxygen uptake was main-
tained through an increase in fractional oxygen extraction
0 (54).
10 y = 3.23 + 0.23x – 0.0035x2
Changes in maternal oxygen capacity, for which mother
VO2 fetus (mL O2 min–1 kg–1)
and fetus can compensate in the short term, are nevertheless
capable of stunting fetal growth, as shown by observations
in chronically anemic sheep (161). In that study, fetal oxygen
5 delivery was reduced sufficiently to affect not only fetal oxida-
tive metabolism but also fetal growth. A sustained reduction
in maternal hematocrit from day 115 of gestation to day 138,
a week before term, led to a 40% reduction in fetal weight
0 (161).
.
0 10 20 30 40 50 60
Fetal hematocrit (%)
Figure 4 Effect on fetal oxygen delivery (DO2 fetus), oxygen extrac- Maternal Arterial PO2
tion and oxygen uptake (VO2 fetus) of varying the hematocrit of the
fetal lamb by exchange transfusion. Reproduced from (55); Copyright Maternal hypoxia
© 1985 with permission from Elsevier. Hypoxic hypoxia at high altitude is discussed below. Other
than at altitude, hypoxic hypoxia is rare in clinical obstetrics,
but it is a potential cause of reduced oxygen delivery to the
their demands. At first inspection these findings suggest that
gravid uterus (136). Fetal responses to maternal hypoxia were
placental oxygen transport is little affected by variations in
studied by Parer (171), who reduced maternal arterial PO2
fetal hematocrit. Therefore it is important to note the close
to about 35 mmHg by allowing the ewe to breathe a gas
correspondence between the normal fetal hematocrit (32%)
mixture low in oxygen. After about 30 min, umbilical blood
and the hematocrit that ensured optimal oxygen delivery to
flow was unchanged, but umbilical venous oxygen content
the fetus. The reduction in oxygen delivery during anemia and
fell from 4.3 to 1.9 mmol L−1 with a resultant 57% decrease
polycythemia could help to explain why higher morbidity and
in oxygen delivery to the fetus. Despite a rise in fractional
mortality rates are associated with these conditions in infants.
oxygen extraction, fetal oxygen uptake fell by 43%. There was
This provides a rationale for treatment of hemolytic and other
gradual development of metabolic acidosis during maternal
forms of anemia by intrauterine transfusion (78, 115).
hypoxia that could be attributed to the accumulation of lactic
acid. This could further compromise fetal oxygenation. In a
setting where maternal hypoxia was maintained for 7 to 8 h,
Oxygen capacity of maternal blood the progressive fall in fetal vascular pH was accompanied by
To examine short-term responses to maternal anemia, Paulone a decrease in umbilical blood flow and led to a reduction in
et al. (173) varied hematocrit between 8% and 30% by fetal oxygen uptake (191).
Volume 5, July 2015 1389
Placental Gas Exchange Comprehensive Physiology
Oxygen supplementation Placental Factors
The opposite situation, maternal hyperoxia, will hardly Placental diffusing capacity for oxygen
improve oxygen delivery to the uterus. Maternal arterial blood
Placental diffusing capacity is defined as the amount of gas
is fully saturated whether the fraction of oxygen in inspired
diffusing across the placental membranes per unit of time per
air is 21% or 100% (the change in dissolved oxygen amounts
unit of partial pressure difference between fetal and mater-
to ca. 0.8 mmol L−1 , an increase of only 10% in blood oxygen
nal blood. It is dependent on the surface area, thickness
content). There may, nevertheless, be an improvement in fetal
and solubility properties of the membranes, the diffusivity
oxygen supply. This is because fetal blood does not normally
of the gas, and the volume of blood in the fetal and mater-
become fully saturated in the placenta. Therefore, if umbilical
nal placental capillaries (124, 132). The standard experimen-
and uterine venous bloods equilibrate at a higher PO2 , there
tal approach is to determine placental diffusing capacity for
can be a considerable improvement in oxygen delivery to the
carbon monoxide (Table 5). Placental diffusing capacity for
fetus (82).
oxygen is about 21% higher than the values obtained for car-
Supplementary oxygen is routinely given during general
bon monoxide (132). The resistance of the interhemal mem-
anesthesia for elective Cesarean section, although current
brane contributes about 60% of the total resistance (132).
evidence suggests it is unnecessary (102). A randomized
The diffusing capacity of the membrane is directly propor-
double-blind study did show an increase in umbilical arterial
tional to the surface area and inversely proportional to the
and venous PO2 and oxygen content when anesthesia was
mean diffusion distance, i.e. mean membrane thickness. Thus,
administered with 100% oxygen (164), confirming a previous
surface area can be estimated from the diffusing capacity
report (177). Although this was in agreement with theoretical
of the interhemal membrane and mean membrane thickness
considerations, the difference was small. The effect of
(132).
supplemental oxygen has also been assessed noninvasively
An alternative approach is to estimate surface area, mem-
by Blood Oxygen Level Dependent magnetic resonance
brane thickness, and vascular volumes by appropriate mor-
imaging. Preliminary findings in healthy pregnancies indi-
phometric techniques and use those values to estimate overall
cated an increase in oxygenation of placental tissue (194)
diffusing capacity and the contributions of each compartment
and some fetal organs, although with no improvement in
in the diffusion pathway (139).
oxygenation of the brain (195).
Could hypoxic, growth-restricted human fetuses benefit
from supplemental oxygen? In one study the value of giving
The interhemal membrane
humidified 55% oxygen to the mother was explored by mea-
suring PO2 in umbilical arterial and venous blood obtained The diffusion distance between fetal and maternal blood
by cordocentesis (165). In four of five fetuses, PO2 values is a limiting factor for oxygen transfer. Across mammals
rose to within the normal range at the end of 10 min of distance is decreased by a reduction in the number of tis-
maternal hyperoxygenation. Later, however, a double-blind sues in the interhemal membrane and thinning of those that
randomized control trial failed to find any beneficial effect of remain (42). Thus, in human placenta, potential tissue lay-
chronic administration of 40% humidified oxygen (116). A ers include the maternal-facing syncytiotrophoblast; cytotro-
recent review by an author of the original study did not rec- phoblasts (Langhans’ layer); connective tissue; and fetal cap-
ommend supplemental oxygen as an effective treatment for illary endothelium. At term, however, cytotrophoblasts are
fetal growth restriction (3). excluded from the exchange areas and a very thin layer of con-
The oxygen content of umbilical venous blood can be nective tissue cytoplasm separates syncytiotrophoblast from
raised by administering hyperbaric oxygen to the mother. In capillary endothelium (Fig. 5). In the epitheliochorial pla-
sheep, administration of 100% oxygen to the ewe at 3 atmo- centa of sheep, there are three additional layers of tissue,
spheres pressure was found to result in pulmonary vasodila- that is, uterine epithelium, connective tissue, and maternal
tion and constriction of the ductus arteriosus (10). Neverthe- capillary endothelium. The diffusion distance is not greatly
less, placental oxygen transfer and fetal oxygen consumption increased, however, because the connective tissue layer is thin,
were maintained (104). Hyperbaric oxygen therapy has been whilst maternal capillaries indent the uterine epithelial cells
recommended for the treatment of carbon monoxide poison- and fetal capillaries indent the trophoblast (42). Indeed, diffu-
ing in pregnancy (210). A recent French study found no dif- sion capacities for the epitheliochorial placenta of the sheep,
ference in psychomotor development between children born endotheliochorial placenta of the dog and hemochorial pla-
following such treatment and matched controls exposed nei- centa of the rhesus monkey are of the same order of magnitude
ther to carbon monoxide nor to hyperbaric oxygen (213). It (Table 5).
should be noted, however, that a fresh Cochrane review failed As discussed below, a reduction in the thickness of the
to find sufficient evidence that hyperbaric oxygen was benefi- interhemal membrane, which should increase diffusing capac-
cial in the treatment of carbon monoxide even in nonpregnant ity, is one of the adaptations that occur in high altitude preg-
adults (31). nancy (139, 185).
1390 Volume 5, July 2015
Comprehensive Physiology Placental Gas Exchange
Table 5 Placental Diffusing Capacity for Carbon Monoxide and Placental Type
Diffusing capacity [mL
Internal structure of min−1 mm Hg−1 kg−1 fetal
Species placenta Interhemal barrier mass (mean ± SEM)] Reference
Rhesus macaque Intervillous space Hemomonochorial 0.65 ± 0.06 (24)
Guinea pig Labyrinth Hemomonochorial 3.27 ± 0.10 (63)
Rabbit Labyrinth Hemodichorial 2.3 ± 0.2 (186)
Rat Labyrinth Hemotrichorial 1.73 ± 0.33 (125)
Dog Interdigitating villi Endotheliochorial 0.57 ± 0.8 (131)
Sheep Interdigitating villi Epitheliochorial 0.55 ± 0.02 (127)
Placental surface area Human pregnancies complicated by fetal growth restric-
tion are associated with reductions in villous tree elaboration
Unexpectedly, values for placental diffusing capacity vary affecting the surface area of the terminal villi (87). This repre-
greatly among species with various types of hemochorial pla- sents a reduction in diffusing capacity, but opinions differ as
centa (Table 5). Values are higher in guinea pig, rat, and rabbit, to whether it is the cause or effect of fetal growth restriction
all of which have labyrinthine placentas with a large counter- (37, 103).
current component. The implication is that the labyrinthine
type of internal structure allows a greater area for placental
exchange (24), which may depend on the compact arrange-
Placental oxygen consumption
ment of the exchange vessels shown by Mossman (160).
Easily overlooked is the high rate of oxygen consumption
by the placenta itself. Although data on human pregnancy is
sparse, it has been determined that the placenta accounts for
40% of the combined fetal and placental oxygen consumption
at term (26). Fetal oxygen consumption in that study was 6.8
mL min−1 kg−1 , which agrees well with a more recent calcu-
lation of 6.58 mL min−1 kg−1 based on direct measurement
of umbilical blood flow and the difference in the umbilical
venous and arterial oxygen content (1).
In agreement, oxygen consumption by the ovine placenta
accounts for 40% of total oxygen uptake by the gravid uterus
(217). In midgestation sheep (71-81 days gestation), where
fetal oxygen consumption is smaller, uteroplacental oxygen
uptake accounts for more than 80% of the total (Table 2) (19).
Fetal capillary
Extrapolating from those experiments, we may expect the
placenta to account for the major part of the combined oxygen
Endothelium
consumption in the second trimester of human pregnancy.
In the ovine placenta, most oxygen is used for oxida-
tive phosphorylation of glucose (141); the remainder likely
is utilized for non-mitochondrial processes. The ATP yield
is expended mainly in protein synthesis and cation transport.
Syncytiotrophoblast Protein synthesis is estimated to account for 30% of placental
oxygen uptake, reflecting the high rates of synthesis of peptide
Intervillous space and steroid hormones. The Na+ -K+ -pump likely accounts for
a further 20% to 30% of placental oxygen use; it serves to
maintain the sodium gradient that is the basis for secondary
active transport of amino acids and other substances (37).
Figure 5 The interhemal barrier of the human placenta. The intervil- Placental oxygen consumption remains remarkably con-
lous space is separated from blood in the fetal capillary by syncytiotro- stant following acute alterations in uterine oxygen supply.
phoblast and fetal capillary endothelium with their basal membranes.
A very thin layer of connective tissue cytoplasm is interposed between This is true both when the oxygen supply is reduced, by par-
the two basal membranes. Courtesy of Dr. Allen C. Enders. tial occlusion of the uterine artery (65, 217), and when it is
Volume 5, July 2015 1391
Placental Gas Exchange Comprehensive Physiology
1600 (A)
1200
800
Oxygen uptake (μmol min–1)
400
0
Fetus Placenta Fetus Placenta
Control Arterial occlusion
2400
(B)
2000
1600
1200
800
400
0
Fetus Placenta Fetus Placenta
Normal growth Growth restricted
Figure 6 Effects of acute and chronic hypoxemia on fetal and placen-
tal oxygen uptake in the sheep. (A) Effect of an acute 60-min reduction Figure 7 Principal pathways of the fetal circulation and representa-
in uterine blood flow on oxygen uptake of the fetus and placenta. Pla-
cental oxygen consumption is maintained at the expense of the fetus. tive values for oxygen saturation of the blood. Well oxygenated blood
Data adapted, from (65). (B) Effect of long-term restriction in uterine oxy- from the umbilical vein (UV) is directed through the ductus venosus (DV)
gen and substrate supply (following carunclectomy) on oxygen uptake (or left lobe of the liver) across the inferior vena cava (IVC), through the
of the fetus and placenta. Placental oxygen consumption is reduced to foramen ovale (FO), left atrium (LA), and ventricle and up the ascending
a greater extent than that of the fetus. Data adapted, from (168). Error aorta (AO) toward the common carotid arteries (CCA). Deoxygenated
bars are SEM. Reproduced, with permssion, from (37); Copyright © blood from the superior vena cava (SVC) and IVC passes through the
2000 with permission from Elsevier. right atrium (RA), right ventricle, pulmonary artery (PA), and ductus arte-
riosus (DA). FOV, foramen ovale valve; LHV, left hepatic vein; MHV,
medial hepatic vein; PV, pulmonary vein; RHV, right hepatic vein. Repro-
duced, with permission, from (105); Copyright © 2004 John Wiley &
Sons, Ltd.
increased, by raising the oxygen saturation of maternal arterial
blood (15). Thus, a reduction of uterine blood flow by 30%
to 50% for 60-min depressed fetal oxygen uptake, because
oxygen consumption by the placenta was maintained at the Oxygen Delivery to Fetal Organs
expense of the fetus (65) (Fig. 6A). At the same time, fetal
glycogen stores were mobilized to supply the placenta with The oxygen content of umbilical venous blood is relatively
glucose and lactate (65). low, but the oxygenated blood is sent preferentially to the
Fetal supply of nutrients to the placenta cannot be sus- fetal heart and brain because it is shunted through the ductus
tained indefinitely. Thus, some form of adaptation can be venosus and foramen ovale (Fig. 7). Rates of blood flow in the
expected during long-term reductions in uterine blood flow. principal vessels have been measured by ultrasound imaging
In the carunclectomy model of fetal growth restriction, where (105). Our knowledge of oxygen saturations in the human
the supply of oxygen and nutrients is restricted throughout fetus is necessarily sparse, but they are assumed to be similar
gestation, uteroplacental oxygen consumption was reduced to those reported for the fetal lamb by Dawes et al. (53).
to a greater extent than fetal oxygen consumption (168) Textbooks of human physiology often repeat their estimates
(Fig. 6B). Consequently, it accounted for a smaller propor- without specifying that the data were obtained in sheep.
tion of total uterine oxygen uptake (28%) than during normal As much as 56% of umbilical venous return passes
growth (53%). Uteroplacental consumption of glucose was through the ductus venosus of the fetal lamb (58, 188). How-
also reduced compared to normal growth controls (168). Pos- ever, estimates of the shunt in human pregnancy, made by
sible mechanisms for limiting placental oxygen consump- Doppler ultrasonography, are 28% to 32% at 18 to 20 weeks
tion are discussed below in the context of high altitude falling to 18% at 31 weeks (107); a second study found a drop
hypoxia. from 40% at 20 weeks to 15% near term (20). The smaller
1392 Volume 5, July 2015
Comprehensive Physiology Placental Gas Exchange
role of the human ductus venosus should not be overempha- accounted for by vascular shunts, including those produced
sized as the remainder of the umbilical venous return passes by mismatching of maternal and fetal placental blood flows.
through the fetal liver, which extracts rather little oxygen; the
oxygen content of hepatic venous blood is quite high (28).
Some species, such as the horse (11) and guinea pig (41),
have disposed of the ductus altogether. The second link in the
Human Pregnancy at High Altitude
shunt is the foramen ovale. Despite anatomical differences Oxygen availability decreases at high altitude because of the
between sheep (7) and human (106), the foramen ovale plays decrease in barometric pressure. At 3100 m (10,200 ft.), the
a similar role in ovine and human fetuses (106, 146). PO2 of the inspired air (PI O2 ) is 98 mm Hg or two-thirds of
The distribution of combined right and left ventricular car- that at sea level. The highest permanent human habitations are
diac output and organ blood flows can be determined in the at about 5000 m, where the PI O2 is 75 mmHg (150). High-
fetal lamb using microspheres (189). There was a redistribu- altitude populations, therefore, offer singular insights about
tion of cardiac output during acute hypoxia in favor of blood the effects of hypoxia and the physiological adaptations that
flow to the brain, myocardium and adrenal glands (47, 190). maintain the oxygen supply to the fetus.
Oxygen delivery to the brain, heart, and adrenals was also Human studies at low and high altitude offer valuable
maintained during acute reductions in uterine blood flow information on the physiology of placental oxygen trans-
(93, 184) or umbilical blood flow (81). There were regional fer and fetal oxygen consumption. They offer some of the
differences within the brain with a redistribution of blood most complete data sets yet available for human pregnancy
flow in favor of critical brain stem areas during acute hypoxia (Table 6).
(9, 174). The neural and endocrine regulation of the fetal cir-
culation, including responses to hypoxia, is the subject of a
separate overview (162). Study populations
Pioneering studies showing an effect of altitude on birth
weight (114) and infant mortality (140) were conducted in
Placental Transfer of Carbon Dioxide Lake County, Colorado, which includes the city of Leadville
3100 m above sea level. This population continues to be a
The fetus produces 0.8 to 0.9 moles of carbon dioxide for valuable research asset (94). The main control population has
each mole of oxygen consumed (144). In the blood, about been Denver, Colorado, at an elevation of 1600 m, but for
8% of the carbon dioxide is in solution, 30% is bound to some recent studies control placentas were collected at sea
hemoglobin as carbaminohemoglobin and the remainder is level in the United Kingdom (48, 221).
transported as bicarbonate ion. Carbon dioxide, not bicar- As many as 140 million people live at altitudes above
bonate, is the major species that crosses the placenta, since 2500 m (153). Some have lived at high altitude for millen-
transfer is scarcely affected by inhibition of carbonic anhy- nia; Tibetans for as many as 25,000 years, Andeans for per-
drase, the intraerythrocytic enzyme that catalyzes conver- haps 13,000 years (151). It has proven particularly instruc-
sion of carbon dioxide and water through carbonic acid to tive to compare these native populations with recent settlers,
hydrogen ion and bicarbonate (129). Because carbon dioxide
is highly lipid soluble, it diffuses rapidly across biological
membranes. Table 6 Some Factors Relevant to Placental Oxygen Transfer in Term
Pregnant women hyperventilate, as first was shown by Human Pregnancy Measured in a Bolivian Population of European
Ancestry Residing at 400 m Above Sea Level (180, 223)
the Danish physiologist Karl Albert Hasselbalch (68). There-
fore, arterial PCO2 is lower in pregnant than in nonpregnant
Variable Value
individuals. In the placenta, oxygenation of fetal hemoglobin
results in decreased affinity for carbon dioxide and PCO2
Uterine blood flow (mL min−1 ) 638 ± 37∗
tends to rise (the Haldane Effect). The opposite occurs dur-
ing deoxygenation of hemoglobin on the maternal side. The Maternal arterial oxygen saturation (%) 97.6 ± 0.1
double Haldane Effect thereby magnifies the PCO2 gradi- Maternal arterial oxygen content (mL L−1 ) 157 ± 2
ent and it accounts for some 46% of carbon dioxide transfer Uterine oxygen delivery (mL min−1 kg−1 fetal mass) 29.7 ± 2.1∗
(71). Therefore, it is counterintuitive that across species the
Umbilical blood flow (mL min−1 ) 325 ± 14∗
PCO2 of umbilical venous blood is 4 to 5 mmHg higher
than that of uterine venous blood (13, 49, 50). This would not Umbilical venous oxygen saturation (%) 52 ± 2
be expected from the venous equilibration model of placen- Umbilical venous oxygen content (mL L−1 ) 103 ± 4
tal gas exchange and indeed the gradient exists even in the Fetal oxygen delivery (mL min−1 kg−1 fetal mass) 9.6 ± 0.5
guinea pig, a species where there is evidence of a substantial
Fetal oxygen uptake (mmol min−1 kg−1 fetus) 6.1 ± 0.3∗
countercurrent component (13). Seeking an explanation by
mathematical modeling, Hill et al. (71) showed the difference ∗ Extrapolated from the figures.
could not be explained by placental metabolism, but could be All values are mean ± SEM.
Volume 5, July 2015 1393
Placental Gas Exchange Comprehensive Physiology
that is, Tibetans with Han Chinese and Andeans with peo- There normally is a fall in maternal blood pressure during
ple of European, mainly Hispanic, descent. The latter studies the second trimester. This does not occur at high altitude even
have been made in both Bolivia and Peru. It is now possi- in women who remain normotensive (169). Preeclampsia, a
ble to test whether individuals have been correctly assigned gestational disease defined in most studies by high blood
to their group using ancestry-informative single nucleotide pressure and proteinuria, is more common at high altitude.
polymorphisms (23, 180). This is desirable as surnames can In Colorado the incidence was 16% at 3100 m compared to
be misleading (196). Bolivia has a substantial population of 3% at 1260 m (169) and in Bolivia 18% at 3600 m versus
Japanese ancestry for which data is available on birth weights 11% at 300 m (101). In both studies, the rates were even
at high and low altitude (100). There is also a small number of higher in primiparous women. Many preeclamptic newborns
studies of high-altitude populations elsewhere, for example, are small for gestational age and preeclampsia can account for
Kirghizstan (185) and Nepal (192). about half the fall in birth weight at high altitude (153). Fetal
The genetic basis for adaptation to life at high alti- distress is more frequent at high altitude (101) and gestational
tude shows similarities and differences between popula- hypertension no doubt contributes to the high infant mortality
tions. There is evidence for positive selection of EGLN1, that was the impetus for the early studies in Leadville (140)
a gene known to be important for oxygen-sensing, in both and persists at troubling levels in Bolivia (101) and elsewhere.
Tibetans and Andeans (23, 133). EGLN1 encodes PHD2, an
enzyme involved in degradation of hypoxia-inducible factor
1α (HIF1α). In contrast, a variant allele of EPAS1, the gene Maternal and fetal adaptations
that encodes HIF2α , is found only in Tibetans and has been Minute ventilation
linked to a blunted erythropoietic response to low ambient
oxygen (18, 77). Single nuclear polymorphisms of EPAS1 Maternal hyperventilation helps preserve arterial oxygena-
in Andeans do not associate with hemoglobin concentration tion during high altitude pregnancy (154). In a comparison
(23). In Andeans, a further two genes associated with oxygen between mothers of smaller babies (<2.9 kg) and mothers of
sensing and vascular control show single nucleotide polymor- larger babies (>3.5 kg), all born at Leadville, Moore et al.
phisms that associate with birth weight (22); EDNRA codes (155) found that the smaller babies were delivered by women
for endothelin receptor type A while PRKAA1 codes for a sub- in whom minute ventilation failed to increase from early to
unit of adenosine monophosphate-activated protein kinase. late gestation. During pregnancy in Andeans, the isocapnic
hypoxic ventilatory response (HVR) increased nearly four-
fold and accounted for a 25% rise in resting ventilation (152).
Birth weight, placental weight, and gestational There are differences between Andeans and Tibetans that
hypertension may affect their ventilatory responses to pregnancy. Tibetans
ventilate more than Andeans at similar altitudes, but whether
Not all babies born at high altitude are small. However, there is a difference in HVR remains unresolved (151). Non-
when corrected for socioeconomic and other risk factors, birth pregnant Tibetans have an HVR similar to that of acclimatized
weight decreases by 102 g for each 1000 m gain in altitude Han (151) and during pregnancy show a similar rise in minute
(94). The critical altitude at which this sets in is 2000 m ventilation and HVR (156).
(159). The decline is steeper in recent residents than in those
with a high-altitude ancestry (Table 7) (97, 153). Birth length
decreases with altitude and here there is no protective effect Hemoglobin concentration
of highland ancestry (196). Placental weight does not change
The decrease in maternal blood hemoglobin concentration
with altitude (84, 180, 208).
that occurs during pregnancy at low altitude was retained in
native Tibetans, whereas in Han at similar altitude hemoglobin
Table 7 Effect of Ancestry and Altitude on Birth Weight in Four did not change. As a result arterial oxygen content was lower
Populations
in Tibetan than in Han women (154 vs. 174 mL −1 ) (156). It is
plausible to link the response of Tibetans to the EPAS1 variant
Decline in Birth weight at 4000 m
described above. Hemoglobin concentration and arterial oxy-
birth weight compared to sea level
Population (g 1000 m−1 ) average (g) gen content increased to similar levels in pregnant Andeans
and Europeans at high altitude (CaO2 178 vs. 187 mL L−1 )
Tibetan (including 88 −296 (223).
Sherpa)
Han 153 −723
Uterine blood flow and oxygen delivery
Andean 89 −338
Uterine artery blood flow can be estimated by measuring bilat-
European 119 −439
eral vessel diameters and flow velocities. An early attempt
Data are from Moore et al. (2011) (153) and were derived by regres- comparing women at Leadville and Denver showed a decrease
sion analysis of data for 4,690,093 newborns. in arterial diameter, increased flow velocity and overall a
1394 Volume 5, July 2015
Comprehensive Physiology Placental Gas Exchange
(A) Low altitude (B) High altitude
Uterine artery blood flow (mL min–1)
Uterine artery blood flow (mL min–1)
900 900
Time, P < 0.001 (both groups) Time, P < 0.001 (both groups)
800 Ancestry, p = NS 800 Ancestry, P < 0.001 Andean
700 Interaction (time*ancestry), NS 700 Interaction (time*ancestry), NS †
600 600 *
500 500
European *
400 400
300 300 European
200 Andean 200
*
100 100
0 0
Non pregnant 20 weeks 36 weeks Non pregnant 20 weeks 36 weeks
Week of pregnancy Week of pregnancy
Figure 8 Uterine artery blood flow at low and high altitude in women of European and Andean descent. (A) At low altitude, the pregnancy-
associated rise in uterine blood flow was similar in Andean and European women. (B) At high altitude, the pregnancy-associated rise in uterine
blood flow was greater in Andeans than in Europeans, resulting in blood flows that were more than one-third larger at 20 or 38 weeks in Andean
women. Error bars are SEM. Asterisks, P < 0.05. Reproduced, with permission, from (98); Copyright © 2009 The American Physiological Society.
decrease in uterine blood flow at the higher elevation (222). in both groups at high altitude, was a reduction in umbilical
In a similar context remodeling of the uterine spiral arter- vein diameter and blood flow. This was largely compensated
ies was found to be reduced at the higher altitude (208). by increased fetal hemoglobin concentration and a leftward
When Andeans and Europeans were compared at low alti- shift in the oxygen dissociation curve contingent on a lower
tude, there was no difference in uterine blood flow (98). At PCO2 (Bohr Effect). As a result fetal oxygen delivery did
high altitude, however, Andeans were able to increase uterine not change with altitude in either Andeans or Europeans, nor
artery blood flow and uteroplacental oxygen delivery at 20 did fetal oxygen consumption when calculated as mL O2
and 36 weeks whereas Europeans did not (Fig. 8); in part this min−1 kg−1 fetal mass. In both groups, however, there was
could be explained by the greater uterine artery diameter of the expected decrement in birth weight.
Andeans (98). Therefore, it is of interest that one genotype
of the PRKAA1 gene, which occurred at higher frequency
in Andeans than Europeans, was associated with increased Placental adaptations
uterine artery diameter (22). A comparison of Tibetan and Interhemal membrane and placental diffusing
Han pregnancies at high altitude reinforces the notion that capacity
increased uterine artery diameter and flow velocity are impor-
A reduction in placental weight with increasing altitude
tant adaptations that serve to maintain uteroplacental oxygen
was seen in a material from Kirghizstan (185), but not in
delivery in populations with highland ancestry (156).
more extensive studies from Colorado (208) and the Andes
In contrast, another recent study found that uterine artery
(84, 180). A comprehensive morphometric study of placen-
diameter, flow velocity, and uterine blood flow decreased at
tas from Bolivia found effects related to altitude irrespective
high altitude both in Andeans and Europeans (223). This was
of ancestry (Andean versus European or Mestizo) or sex of
partly compensated by increased hemoglobin concentration
the newborn. At high altitude there was a reduction in vil-
and arterial oxygen content; in relation to fetal mass, uteropla-
lous volume and surface area (83). The mean thickness of the
cental oxygen delivery (mL min−1 kg−1 ) was not different at
interhemal membrane was reduced, due in part to the greater
altitude (223). Differences between the findings may depend
proximity of fetal capillaries to the overlying trophoblast; this
on study design [discussed in (196)].
reduced the effective diffusion distance (85,86,139). A reduc-
tion in the thickness of the interhemal membrane, resulting
Umbilical blood flow and oxygen delivery to the in increased morphometric diffusing capacity, was also found
in Kirghizstan and interpreted as a placental adaptation to
fetus
high-altitude pregnancy (185).
Ultrasound can be used to estimate umbilical venous blood
flow. When paired with measurement of blood oxygen content
Placental oxygen consumption
in the umbilical artery and vein, made at Cesarean section,
oxygen delivery to and consumption by the fetus can be cal- Several recent studies sought for an explanation of the
culated. This was done in conjunction with the above study reduced villous volume in high-altitude placentas in terms of
on Andean and European pregnancies at low and high alti- endoplasmic reticulum stress and reduced protein synthesis.
tude (180). The most pronounced difference, which occurred These papers compared placentas from Leadville (elevation
Volume 5, July 2015 1395
Placental Gas Exchange Comprehensive Physiology
3100 m) with others collected in Cambridge and London (sea (A)
level). At sea level, placentas collected after vaginal delivery P < 0.0001
showed evidence of hypoxic stress compared to those from 4 Venous
Umbilical plasma glucose
Cesarean section. This difference was not seen at altitude P < 0.0001 Arterial
and its lack was interpreted as evidence of hypoxic precondi- 3
(mmol L–1)
tioning (207). Further experiments indicated the presence of
2
endoplasmic reticulum stress in high altitude placentas (221).
It was then shown that expression of the HIF-1α-responsive 1
microRNA-210 (miR-210) was increased in high altitude pla-
centas; miR-210 has been implicated in downregulation of 0
mitochondrial oxygen consumption. It was further suggested,
based on work with cell lines, that inhibition of protein syn- 400 3600 m
(B)
thesis altered mitochondrial function by suppressing com-
plexes I and IV of the electron transport chain (48). Protein
Umbilical ΔFV-FA glucose
1.0
synthesis has been estimated to account for about 30% of
placental oxygen uptake (37). Thus, overlapping mechanisms 0.8
(mmol L–1)
may act on the hypoxic placenta to suppress its oxygen con- 0.6
sumption at the level of the mitochondrial electron transport
0.4
chain (48).
Although the placenta may adapt to spare available oxy- 0.2
gen for fetal use, this could have a negative effect on fetal 0.0
growth. The aforementioned studies of Andean and European
pregnancies at low- and high-altitude included measurements 400 3600 m
of blood glucose concentration and fetal glucose uptake (224). (C)
Changes at altitude were similar in Andeans and Europeans. P < 0.01
(μmol min–1 kg–1 birth weight)
Although uteroplacental glucose delivery seemed not to be
Fetal glucose consumption
80
compromised, glucose concentrations were lower in umbili-
cal venous and arterial blood and fetal glucose uptake reduced 60
by 28% (Fig. 9). It was suggested that anaerobic consumption
40
of glucose by the placenta limited glucose availability to the
fetus. There was also a reduction in expression of the glucose 20
transporter GLUT1 at the basal membrane of the syncytiotro-
phoblast, which was seen as a secondary effect (224). 0
Overall, current thinking points to high altitude hypoxia
acting primarily at the level of the placenta, reducing mito- 400 3600 m
chondrial respiration and protein synthesis and thus passing Figure 9 Plasma glucose concentrations in umbilical vessels and
more of the available oxygen to the fetus. Conversely, the pla- fetal glucose uptake in term human pregnancies at low (400 m) and
centa maintains a high consumption of glucose, restricting its high (3600 m) altitude. (A) Umbilical arterial and venous plasma glu-
availability to the fetus and leading ultimately to restriction cose concentrations were lower at high than at low altitude. (B) The
fetal venous-to-arterial plasma glucose concentration difference (ΔFV-
of fetal growth. FA) was similar at low and high altitude. (C) Fetal glucose consumption
(corrected for birth weight) was greater at low than at high altitude.
Error bars are SEM. Reproduced, with permission, from (224); Copy-
right © 2010 Zamudio et al.
Animal models of high-altitude pregnancy
Sheep
Pioneering studies on sheep indigenous to Andean pastures changes occurred in placentome shape and vessel branch-
(4500 m) found they had raised fetal hematocrits whilst umbil- ing and were interpreted as placental adaptations to hypoxia
ical venous and arterial PO2 were similar to sea level values (110, 176). More recent studies have revealed that chronic
(145, 183). The logistics of performing more sophisticated hypoxia can adversely affect vascular tone in upstream vessels
studies at altitude are demanding and usually involve bring- by inhibiting the steroid-mediated upregulation of potassium
ing the sheep to a lower altitude laboratory. Fetal responses to channels in uterine artery smooth muscle cells (225, 226).
high-altitude hypoxia were studied in this way by comparing An alternative approach is to keep pregnant sheep in a
sheep that had been kept at the White Mountain Research Sta- hypobaric chamber. When ewes were kept at an ambient pres-
tion in California (elevation 3820 m) with those kept through- sure of 429 mmHg (equivalent to an altitude of 4572 m) from
out at sea level (99,175). In these studies, there was no effect of 30 to 135 days gestation, average fetal weight was 21% lower
sojourn at high altitude on fetal or placental weight although than for control pregnancies (88). During hypobaric hypoxia
1396 Volume 5, July 2015
Comprehensive Physiology Placental Gas Exchange
of shorter duration, from 120 to 141 days gestation, fetal arte- oxygen uptake by the llama fetus (4.8 mL min−1 kg−1 ) is
rial oxygen saturation remained low, but this was compen- close to the range of values reported for the sheep fetus (21).
sated by a gradual rise in hemoglobin concentration. There Cardiac output and organ blood flows are relatively low in
was nevertheless a 17% reduction in fetal body weight (88). the llama fetus but oxygen extraction is more efficient (121).
Thus the long-term effect of hypobaric hypoxia in sheep is to When pregnant animals were moved from sea level to 4400
slow fetal growth. m, PO2 in the descending aorta of the fetus dropped from 21
to 15 mmHg with no change in blood pressure or heart rate
but a considerable increase in blood flow to the heart (122).
Llama Similarly, when pregnant llamas at sea level were allowed to
South American camelids with a long history of residence breathe a gas mixture with a low oxygen fraction, myocardial
on the Andean altiplano include the llama (Lama glama). blood flow tripled (119). In contrast to the fetal lamb, however,
Adaptations to high altitude include a higher blood oxygen there was no change in blood flow to the brain (119). A
affinity that is conserved in pregnant animals both at high decrease in oxygen delivery to the cerebral hemispheres was
altitude [4500 m (143)] and when they are brought closer largely compensated by increased extraction, although after
to sea level (158) (Fig. 10). In contrast, fetal llamas have 60 min of hypoxia there was also a fall in cerebral oxygen
a higher hemoglobin concentration than fetal lambs (158) consumption (123).
and thus a higher blood oxygen capacity (21). The estimated
Guinea pig
(A)
100 The laboratory guinea pig (Cavia porcellus) stems from a
species domesticated in the Andes (C. tschudii) and imported
to Europe in the 17th Century (197). Pregnant guinea pigs have
been kept in a hypobaric chamber simulating high altitude
Hemoglobin saturation (%)
75
(3962 m) and compared with those kept at 1600 m in Denver
(215). These experiments focused on the impact of hypobaric
Fetal IIamas hypoxia on the adaptation of the uterine arteries to pregnancy
50
Maternal IIamas and revealed alterations at both the structural and functional
level (187, 215, 216). As in several human studies, simulated
high altitude in guinea pigs led to a decrease in fetal weight
25 with no change in placental weight (187).
0
0 10 20 30 40 50 60 70 80 90 100 Conclusion
Po2 (Torr)
The fetus is adapted to a low-oxygen environment. Umbilical
(B) venous PO2 is about 30 mmHg and PO2 is even lower in the
100
blood reaching the tissues. Blood oxygen content is higher
than these values imply because of the high hematocrit and
greater oxygen affinity of fetal hemoglobin. Perhaps surpris-
Hemoglobin saturation (%)
75
ingly, the normally grown fetus has a large reserve capacity.
The experiments summarized in Table 8 show that fetal oxy-
Fetal sheep gen uptake is maintained when oxygen delivery is reduced by
50 half. Fractional oxygen extraction is increased with a resul-
Maternal sheep
tant drop in oxygen content of umbilical arterial blood and
there is a corresponding increase in oxygen uptake across the
25 placenta. As a further example, reduction of uterine blood
flow, and thus of uteroplacental oxygen delivery, led to a 54%
decrease in fetal oxygen delivery; fetal oxygen uptake was
0 maintained, however, with a drop in the oxygen content of
0 10 20 30 40 50 60 70 80 90 100 umbilical arterial blood from 4 to 2 mmol L−1 (217). It must
Po2 (Torr) be stressed that these are short term responses to hypoxia.
They are nevertheless indicative of fetal resilience to acute
Figure 10 Blood oxygen dissociation curves of maternal and fetal
episodes of hypoxia such as those occurring during labor.
blood of llamas (upper panel) and sheep (lower panel). Maternal blood
has a relatively high oxygen affinity in the llama. Reproduced, with per- A reduction in oxygen delivery greater than 50% is not
mission, from (158); Copyright © 1996 with permission from Elsevier. so well tolerated. When fetal oxygen delivery falls below a
Volume 5, July 2015 1397
Placental Gas Exchange Comprehensive Physiology
Table 8 Effect on Fetal Oxygen Delivery, Fractional Oxygen Extraction and Fetal Oxygen Uptake of a Short-Term 50%
Reduction in Some Parameters of Importance for Placental Gas Exchange
Change (% control value)
Fractional O2
Variable Fetal O2 delivery extraction Fetal O2 uptake Reference
Umbilical blood flow −46% +55% −18% (80)
Umbilical blood flow −50% +55% −23% (57)
Fetal hematocrit −49% +92% −14% (55)
Maternal hematocrit −50% +41% −27% (173)
Fetal blood O2 affinity1 −64% +57% −44% (79)
1 Umbilical blood flow fell by 33%.
critical level, aerobic metabolism can no longer be maintained 10
and the fetus becomes acidemic (Fig. 11) (56).
A quite different picture emerges when hypoxia is main-
Fetal O2 consumption
(mL O2 min–1 kg–1)
tained for longer periods of time (Table 9). Typically, this
leads to reduction in the rate of fetal growth. Fetal acidemia is
slight or absent, suggesting the fetus is able to maintain aer- 5
obic metabolism. It was shown in the carunclectomy model
that while fetal oxygen uptake decreased in the small fetuses
(from 1.1 to 0.6 mmol min−1 ), it was unchanged when cor-
rected for fetal mass (0.395 to 0.355 mmol−1 min−1 kg−1 )
(168). Placental weight was little affected except in the carun- 0
clectomy and embolization models where it was the object of
the insult (Table 9). The results of these sheep experiments 10
are in agreement with what is known from human pregnancy
at high altitude. Moreover, they have broader implications for
human pregnancy. Maintenance of an adequate oxygen deliv-
ery to the intervillous space of the placenta depends on the
Base excess (mEq L–1)
0
physiological transformation of the uterine spiral arteries by
the extravillous trophoblast (67, 178). When this process is
defective, a number of pregnancy complications can ensue,
most notably fetal growth restriction and preeclampsia (30). –10
The most promising scientific developments of recent date
concern the central role of the placenta. It has been clear for
some time that the placenta has a high oxygen consumption
that is maintained during acute hypoxia (Fig. 6A). Conversely, –20
during long-term reduction in oxygen delivery to the gravid
uterus, placental oxygen consumption is reduced in favor of 0
the fetus (Fig. 6B). Moreover, as discussed above, the more 0 10 20 30
moderate impact of hypoxia on placental mass belies the Fetal O2 delivery (mL O2 min–1 kg–1)
fact that there are structural and functional changes in the
placenta of sheep and at high altitude in human pregnancy. Figure 11 Fetal oxygen consumption (upper panel) and arterial
blood base excess (lower panel) as a function of fetal oxygen delivery
Changes in villus development are associated also with fetal in sheep. Fetal oxygen uptake remained constant until oxygen delivery
growth restriction and preeclampsia (103). It now appears that was reduced below ca. 13 mL min−1 kg−1 fetal mass (0.6 mmol min−1
hypoxia can directly impact the placenta, causing endoplas- kg−1 ). There was then an increase in anaerobic metabolism with a resul-
tant fall in arterial base excess. Data are from experiments in which both
mic reticulum stress, inhibition of protein synthesis, and sup- oxygen affinity (hemoglobin type) and oxygen capacity (hemoglobin
pression of oxygen consumption in the mitochondrial electron concentration) were varied. Circles: fetal hemoglobin; squares: adult
transport chain (48, 221). The evidence is convincing in rela- hemoglobin; filled circles and squares: normal hematocrit; half-filled cir-
cles and squares: moderate anemia; open circles and squares: severe
tion to high altitude hypoxia [“preplacental hypoxia” (103)] anemia. Reproduced, with permission, from (56); Copyright © 1989
and should stimulate further research in the context of reduced with permission from Elsevier.
1398 Volume 5, July 2015
Comprehensive Physiology Placental Gas Exchange
Table 9 Effect on Fetal and Placental Weights of Long-Term Reductions in Oxygen Delivery to the Fetus
Duration Change (% control value)
Method Total (days) Gestation (days) Fetal weight Placental weight Reference
Umbilical blood flow reduced by embolization 10 Late gestation −13% (NS) −22% (61)
Uterine blood flow clamped 25 113-138 −21% −9% (112)
Maternal anemia 28 110-138 −40% N/A (161)
Hypobaric hypoxia 105 30-135 −21% −23% (NS) (88)
Carunclectomy 130 0-130 −31% −51% (168)
intervillous blood flow and fetal growth restriction [“uteropla- 16. Bauer C, Ludwig M, Ludwig I, Bartels H. Factors governing the oxygen
cental hypoxia” (103)]. Another interesting hypothesis, aris- affinity of human adult and foetal blood. Respir Physiol 7: 271-277,
1969.
ing from high altitude studies, is that the placenta increases 17. Bauer C, Tamm R, Petschow D, Bartels R, Bartels H. Oxygen affinity
anaerobic consumption of glucose and deprives the fetus of and allosteric effects of embryonic mouse haemolglobins. Nature 257:
333-334, 1975.
substrate, thereby slowing fetal growth (224). A good deal is 18. Beall CM, Cavalleri GL, Deng L, Elston RC, Gao Y, Knight J, Li C,
known about placental and fetal handling of glucose in sheep Li JC, Liang Y, McCormack M, Montgomery HE, Pan H, Robbins PA,
Shianna KV, Tam SC, Tsering N, Veeramah KR, Wang W, Wangdui
(69,70) and this topic deserves to be revisited in the context of P, Weale ME, Xu Y, Xu Z, Yang L, Zaman MJ, Zeng C, Zhang L,
hypoxia, not least because the resultant fetal responses may Zhang X, Zhaxi P, Zheng YT. Natural selection on EPAS1 (HIF2alpha)
associated with low hemoglobin concentration in Tibetan highlanders.
impact adult health (205). Proc Natl Acad Sci U S A 107: 11459-11464, 2010.
19. Bell AW, Kennaugh JM, Battaglia FC, Makowski EL, Meschia G.
Metabolic and circulatory studies of fetal lamb at midgestation. Am J
Physiol 250: E538-E544, 1986.
20. Bellotti M, Pennati G, De GC, Battaglia FC, Ferrazzi E. Role of ductus
References venosus in distribution of umbilical blood flow in human fetuses during
second half of pregnancy. Am J Physiol Heart Circ Physiol 279: H1256-
1. Acharya G, Sitras V. Oxygen uptake of the human fetus at term. Acta H1263, 2000.
Obstet Gynecol Scand 88: 104-109, 2009. 21. Benavides CE, Perez R, Espinoza M, Cabello G, Riquelme R, Parer
2. Aguileta G, Bielawski JP, Yang Z. Proposed standard nomenclature for JT, Llanos AJ. Cardiorespiratory functions in the fetal llama. Respir
the alpha- and beta-globin gene families. Genes Genet Syst 81: 367-371, Physiol 75: 327-334, 1989.
2006. 22. Bigham AW, Julian CG, Wilson MJ, Vargas E, Browne VA, Shriver
3. Alberry M, Soothill P. Management of fetal growth restriction. Arch MD, Moore LG. Maternal PRKAA1 and EDNRA genotypes are asso-
Dis Child Fetal Neonatal Ed 92: F62-F67, 2007. ciated with birth weight, and PRKAA1 with uterine artery diameter and
4. Alexander G. Studies on the placenta of the sheep (Ovis aries l.). Effect metabolic homeostasis at high altitude. Physiol Genomics 46: 687-697,
of surgical reduction in the number of caruncles. J Reprod Fertil 7: 2014.
307-322, 1964. 23. Bigham AW, Wilson MJ, Julian CG, Kiyamu M, Vargas E, Leon-
5. Ampey BC, Morschauser TJ, Lampe PD, Magness RR. Gap junction Velarde F, Rivera-Chira M, Rodriquez C, Browne VA, Parra E, Brutsaert
regulation of vascular tone: Implications of modulatory intercellular TD, Moore LG, Shriver MD. Andean and Tibetan patterns of adaptation
communication during gestation. Adv Exp Med Biol 814: 117-132, to high altitude. Am J Hum Biol 25: 190-197, 2013.
2014. 24. Bissonnette JM, Longo LD, Novy MJ, Murata Y, Martin CB, Jr. Pla-
6. Anderson DF, Faber JJ. Regulation of fetal placental blood flow in the cental diffusing capacity and its relation to fetal growth. J Dev Physiol
lamb. Am J Physiol 247: R567-R574, 1984. 1: 351-359, 1979.
7. Anderson DF, Faber JJ, Morton MJ, Parks CM, Pinson CW, Thornburg 25. Bocking AD, White SE, Homan J, Richardson BS. Oxygen consump-
KL. Flow through the foramen ovale of the fetal and new-born lamb. J tion is maintained in fetal sheep during prolonged hypoxaemia. J Dev
Physiol 365: 29-40, 1985. Physiol 17: 169-174, 1992.
8. Anderson DF, Parks CM, Faber JJ. Fetal O2 consumption in sheep 26. Bonds DR, Crosby LO, Cheek TG, Hagerdal M, Gutsche BB, Gabbe
during controlled long-term reductions in umbilical blood flow. Am J SG. Estimation of human fetal-placental unit metabolic rate by appli-
Physiol 250: H1037-H1042, 1986. cation of the Bohr principle. J Dev Physiol 8: 49-54, 1986.
9. Ashwal S, Majcher JS, Longo LD. Patterns of fetal lamb regional 27. Boyle DW, Lecklitner S, Liechty EA. Effect of prolonged uterine blood
cerebral blood flow during and after prolonged hypoxia: Studies during flow reduction on fetal growth in sheep. Am J Physiol 270: R246-R253,
the posthypoxic recovery period. Am J Obstet Gynecol 139: 365-372, 1996.
1981. 28. Bristow J, Rudolph AM, Itskovitz J, Barnes R. Hepatic oxygen and
10. Assali NS, Kirschbaum TH, Dilts PVJ. Effects of hyperbaric oxy- glucose metabolism in the fetal lamb. Response to hypoxia. J Clin
gen on uteroplacental and fetal circulation. Circ Res 22: 573-588, Invest 71: 1047-1061, 1983.
1968. 29. Brittain T. Molecular aspects of embryonic hemoglobin function. Mol
11. Barnes RJ, Comline RS, Dobson A, Silver M, Burton GJ, Steven DH. Aspects Med 23: 293-342, 2002.
On the presence of a ductus venosus in the fetal pig in late gestation. J 30. Brosens I, Pijnenborg R, Vercruysse L, Romero R. The “Great Obstet-
Dev Physiol 1: 105-110, 1979. rical Syndromes” are associated with disorders of deep placentation.
12. Barry JS, Anthony RV. The pregnant sheep as a model for human Am J Obstet Gynecol 204: 193-201, 2011.
pregnancy. Theriogenology 69: 55-67, 2008. 31. Buckley NA, Juurlink DN, Isbister G, Bennett MH, Lavonas EJ. Hyper-
13. Bartels H, El Yassin D, Reinhardt W. Comparative studies of placental baric oxygen for carbon monoxide poisoning. Cochrane Database Syst
gas exchange in guinea pigs, rabbits and goats. Respir Physiol 2: 149- Rev CD002041, 2011.
162, 1967. 32. Bunn HF. Evolution of mammalian hemoglobin function. Blood 58:
14. Battaglia FC, Meschia G. Review of studies in human pregnancy of 189-197, 1981.
uterine and umbilical blood flows. Med Wieku Rozwoj 17: 287-292, 33. Burton GJ. Oxygen, the Janus gas; its effects on human placental devel-
2013. opment and function. J Anat 215: 27-35, 2009.
15. Battaglia FC, Meschia G, Makowski EL, Bowes W. The effect of 34. Burton GJ, Fowden AL. Review: The placenta and developmental pro-
maternal oxygen inhalation upon fetal oxygenation. J Clin Invest 47: gramming: Balancing fetal nutrient demands with maternal resource
548-555, 1968. allocation. Placenta 33(Suppl): S23-S27, 2012.
Volume 5, July 2015 1399
Placental Gas Exchange Comprehensive Physiology
35. Carter AM. Factors affecting gas transfer across the placenta and the 64. Gluckman PD, Hanson MA, Cooper C, Thornburg KL. Effect of in
oxygen supply to the fetus. J Dev Physiol 12: 305-322, 1989. utero and early-life conditions on adult health and disease. N Engl J
36. Carter AM. Current topic: Restriction of placental and fetal growth in Med 359: 61-73, 2008.
the guinea-pig. Placenta 14: 125-135, 1993. 65. Gu W, Jones CT, Parer JT. Metabolic and cardiovascular effects on
37. Carter AM. Placental oxygen consumption. Part I: In vivo studies—A fetal sheep of sustained reduction of uterine blood flow. J Physiol 368:
review. Placenta 21 (Suppl A): S31-S37, 2000. 109-129, 1985.
38. Carter AM. Animal models of human placentation—A review. Placenta 66. Hafez SA, Borowicz P, Reynolds LP, Redmer DA. Maternal and fetal
28(Suppl A): S41-S47, 2007. microvasculature in sheep placenta at several stages of gestation. J Anat
39. Carter AM. Evolution of placental function in mammals: The molecular 216: 292-300, 2010.
basis of gas and nutrient transfer, hormone secretion, and immune 67. Harris LK. IFPA Gabor Than Award lecture: Transformation of the spi-
responses. Physiol Rev 92: 1543-1576, 2012. ral arteries in human pregnancy: Key events in the remodelling timeline.
40. Carter AM, Challis JR, Svendsen P. Regional adrenal blood flow Placenta 32 (Suppl 2): S154-S158, 2011.
responses to adrenocorticotropic hormone after chronic embolization 68. Hasselbalch KA. Ein Beitrag zur Respirationsphysiologie der Gra-
of the fetal placental circulation in sheep. J Endocrinol 148: 517-522, vidität. Scand Arch Physiol 27: 1-12, 1912.
1996. 69. Hay WW, Jr. Placental-fetal glucose exchange and fetal glucose
41. Carter AM, Detmer A, Egund N. Contribution of the umbilical and metabolism. Trans Am Clin Climatol Assoc 117: 321-339, 2006.
portal veins to the hepatic blood supply of guinea pig fetuses—An 70. Hay WW, Jr, Molina RA, DiGiacomo JE, Meschia G. Model of pla-
angiographic study. Lab Anim Sci 42: 174-179, 1992. cental glucose consumption and glucose transfer. Am J Physiol 258:
42. Carter AM, Enders AC. Comparative aspects of trophoblast develop- R569-R577, 1990.
ment and placentation. Reprod Biol Endocrinol 2: 46, 2004. 71. Hill EP, Power GG, Longo LD. A mathematical model of carbon diox-
43. Carter AM, Enders AC. The evolution of epitheliochorial placentation. ide transfer in the placenta and its interaction with oxygen. Am J Physiol
Annu Rev Anim Biosci 1: 443-467, 2013. 224: 283-299, 1973.
44. Carter AM, Mess A. Mammalian placentation: Implications for animal 72. Hofmann O, Mould R, Brittain T. Allosteric modulation of oxygen
models. In: McManus LM, Mitchell R, editors. Pathobiology of Human binding to the three human embryonic haemoglobins. Biochem J 306(Pt
Disease. San Diego: Elsevier, 2014, pp. 2423-2443. 2): 367-370, 1995.
45. Chase AR, Sohal M, Howard J, Laher R, McCarthy A, Layton DM, 73. Holland HD. The oxygenation of the atmosphere and oceans. Philos
Oteng-Ntim E. Pregnancy outcomes in sickle cell disease: A retrospec- Trans R Soc Lond B Biol Sci 361: 903-915, 2006.
tive cohort study from two tertiary centres in the UK. Obstet Med 3: 74. Holland RA, Calvert SJ. Oxygen transport by rabbit embryonic blood:
110-112, 2010. High cooperativity of hemoglobin-oxygen binding. Respir Physiol 99:
46. Clapp JF, III. The relationship between blood flow and oxygen uptake 157-164, 1995.
in the uterine and umbilical circulations. Am J Obstet Gynecol 132: 75. Hooper SB, Walker DW, Harding R. Oxygen, glucose, and lactate
410-413, 1978. uptake by fetus and placenta during prolonged hypoxemia. Am J Physiol
47. Cohn HE, Sacks EJ, Heymann MA, Rudolph AM. Cardiovascular 268: R303-R309, 1995.
responses to hypoxemia and acidemia in fetal lambs. Am J Obstet 76. Howard J, Oteng-Ntim E. The obstetric management of sickle cell
Gynecol 120: 817-824, 1974. disease. Best Pract Res Clin Obstet Gynaecol 26: 25-36, 2012.
48. Colleoni F, Padmanabhan N, Yung HW, Watson ED, Cetin I, Tissot 77. Huerta-Sanchez E, Jin X, Asan, Bianba Z, Peter BM, Vinckenbosch
van Patot MC, Burton GJ, Murray AJ. Suppression of mitochondrial N, Liang Y, Yi X, He M, Somel M, Ni P, Wang B, Ou X, Huasang,
electron transport chain function in the hypoxic human placenta: A role Luosang J, Cuo ZX, Li K, Gao G, Yin Y, Wang W, Zhang X, Xu
for miRNA-210 and protein synthesis inhibition. PLoS One 8: e55194, X, Yang H, Li Y, Wang J, Wang J, Nielsen R. Altitude adaptation in
2013. Tibetans caused by introgression of Denisovan-like DNA. Nature 512:
49. Comline RS, Silver M. PO2 , PCO2 and pH levels in the umbilical and 194-197, 2014.
uterine blood of the mare and ewe. J Physiol 209: 587-608, 1970. 78. Illanes S, Soothill P. Management of red cell alloimmunisation in preg-
50. Comline RS, Silver M. A comparative study of blood gas tensions, oxy- nancy: The non-invasive monitoring of the disease. Prenat Diagn 30:
gen affinity and red cell 2,3 DPG concentrations in foetal and maternal 668-673, 2010.
blood in the mare, cow and sow. J Physiol 242: 805-826, 1974. 79. Itskovitz J, Goetzman BW, Roman C, Rudolph AM. Effects of fetal-
51. Conrad KP, Benyo DF, Westerhausen-Larsen A, Miles TM. Expression maternal exchange transfusion on fetal oxygenation and blood flow
of erythropoietin by the human placenta. FASEB J 10: 760-768, 1996. distribution. Am J Physiol 247: H655-H660, 1984.
52. Davis LE, Widness JA, Brace RA. Renal and placental secretion of 80. Itskovitz J, LaGamma EF, Rudolph AM. The effect of reducing umbili-
erythropoietin during anemia or hypoxia in the ovine fetus. Am J Obstet cal blood flow on fetal oxygenation. Am J Obstet Gynecol 145: 813-818,
Gynecol 189: 1764-1770, 2003. 1983.
53. Dawes GS, Mott JC, Widdicombe JG. The foetal circulation in the 81. Itskovitz J, LaGamma EF, Rudolph AM. Effects of cord compression
lamb. J Physiol 126: 563-587, 1954. on fetal blood flow distribution and O2 delivery. Am J Physiol 252:
54. Delpapa EH, Edelstone DI, Milley JR, Balsan M. Effects of chronic H100-H109, 1987.
maternal anemia on systemic and uteroplacental oxygenation in near- 82. Jackson BT, Piasecki GJ, Novy MJ. Fetal responses to altered maternal
term pregnant sheep. Am J Obstet Gynecol 166: 1007-1012, 1992. oxygenation in rhesus monkey. Am J Physiol 252: R94-101, 1987.
55. Edelstone DI, Caine ME, Fumia FD. Relationship of fetal oxygen 83. Jackson MR, Mayhew TM, Haas JD. Morphometric studies on villi in
consumption and acid-base balance to fetal hematocrit. Am J Obstet human term placentae and the effects of altitude, ethnic grouping and
Gynecol 151: 844-851, 1985. sex of newborn. Placenta 8: 487-495, 1987.
56. Edelstone DI, Darby MJ, Bass K, Miller K. Effects of reductions in 84. Jackson MR, Mayhew TM, Haas JD. The volumetric composition of
hemoglobin-oxygen affinity and hematocrit level on oxygen consump- human term placentae: Altitudinal, ethnic and sex differences in Bolivia.
tion and acid-base state in fetal lambs. Am J Obstet Gynecol 160: J Anat 152: 173-187, 1987.
820-826, 1989. 85. Jackson MR, Mayhew TM, Haas JD. On the factors which contribute to
57. Edelstone DI, Peticca BB, Goldblum LJ. Effects of maternal oxy- thinning of the villous membrane in human placentae at high altitude.
gen administration on fetal oxygenation during reductions in umbil- I. Thinning and regional variation in thickness of trophoblast. Placenta
ical blood flow in fetal lambs. Am J Obstet Gynecol 152: 351-358, 9: 1-8, 1988.
1985. 86. Jackson MR, Mayhew TM, Haas JD. On the factors which contribute to
58. Edelstone DI, Rudolph AM, Heymann MA. Liver and ductus venosus thinning of the villous membrane in human placentae at high altitude.
blood flows in fetal lambs in utero. Circ Res 42: 426-433, 1978. II. An increase in the degree of peripheralization of fetal capillaries.
59. Fisher DE, Paton JB, Peterson EN, Delannoy CW, Behrman RE. Umbil- Placenta 9: 9-18, 1988.
ical blood flow, fetal oxygen consumption and placental diffusion 87. Jackson MR, Walsh AJ, Morrow RJ, Mullen JB, Lye SJ, Ritchie JW.
clearance of antipyrine in the baboon. Respir Physiol 15: 141-150, Reduced placental villous tree elaboration in small-for-gestational-age
1972. pregnancies: Relationship with umbilical artery Doppler waveforms.
60. Fujikura T, Yoshida J. Blood gas analysis of placental and uterine blood Am J Obstet Gynecol 172: 518-525, 1995.
during cesarean delivery. Obstet Gynecol 87: 133-136, 1996. 88. Jacobs R, Robinson JS, Owens JA, Falconer J, Webster ME. The effect
61. Gagnon R, Johnston L, Murotsuki J. Fetal placental embolization in the of prolonged hypobaric hypoxia on growth of fetal sheep. J Dev Physiol
late-gestation ovine fetus: Alterations in umbilical blood flow and fetal 10: 97-112, 1988.
heart rate patterns. Am J Obstet Gynecol 175: 63-72, 1996. 89. Jauniaux E, Hempstock J, Teng C, Battaglia FC, Burton GJ. Polyol
62. Gagnon R, Murotsuki J, Challis JR, Fraher L, Richardson BS. Fetal concentrations in the fluid compartments of the human conceptus during
sheep endocrine responses to sustained hypoxemic stress after chronic the first trimester of pregnancy: Maintenance of redox potential in a
fetal placental embolization. Am J Physiol 272: E817-E823, 1997. low oxygen environment. J Clin Endocrinol Metab 90: 1171-1175,
63. Gilbert RD, Cummings LA, Juchau MR, Longo LD. Placental diffusing 2005.
capacity and fetal development in exercising or hypoxic guinea pigs. J 90. Jauniaux E, Watson AL, Hempstock J, Bao YP, Skepper JN, Burton
Appl Physiol Respir Environ Exerc Physiol 46: 828-834, 1979. GJ. Onset of maternal arterial blood flow and placental oxidative stress.
1400 Volume 5, July 2015
Comprehensive Physiology Placental Gas Exchange
A possible factor in human early pregnancy failure. Am J Pathol 157: 118. Link G, Clark KE, Lang U. Umbilical blood flow during pregnancy:
2111-2122, 2000. Evidence for decreasing placental perfusion. Am J Obstet Gynecol 196:
91. Jelkmann W, Bauer C. Embryonic hemoglobins: Dependency of func- 489-7, 2007.
tional characteristics on tetramer composition. Pflugers Arch 377: 75- 119. Llanos A, Riquelme R, Sanhueza E, Gaete C, Cabello G, Parer J. Car-
80, 1978. diorespiratory responses to acute hypoxemia in the chronically catheter-
92. Jelkmann W, Bauer C. 2,3-DPG levels in relation to red cell enzyme ized fetal llama at 0.7-0.9 of gestation. Comp Biochem Physiol A Mol
activities in rat fetuses and hypoxic newborns. Pflugers Arch 389: 61-68, Integr Physiol 119: 705-709, 1998.
1980. 120. Llanos AJ, Ebensperger G, Herrera EA, Reyes RV, Pulgar VM, Seron-
93. Jensen A, Roman C, Rudolph AM. Effects of reducing uterine blood Ferre M, Diaz M, Parer JT, Giussani DA, Moraga FA, Riquelme RA.
flow on fetal blood flow distribution and oxygen delivery. J Dev Physiol Fetal and postnatal pulmonary circulation in the Alto Andino. Placenta
15: 309-323, 1991. 32(Suppl 2): S100-S103, 2011.
94. Jensen GM, Moore LG. The effect of high altitude and other risk factors 121. Llanos AJ, Riquelme RA, Herrera EA, Ebensperger G, Krause B, Reyes
on birthweight: Independent or interactive effects? Am J Public Health RV, Sanhueza EM, Pulgar VM, Behn C, Cabello G, Parer JT, Giussani
87: 1003-1007, 1997. DA, Blanco CE, Hanson MA. Evolving in thin air—Lessons from the
95. Johnson RM, Prychitko T, Gumucio D, Wildman DE, Uddin M, llama fetus in the altiplano. Respir Physiol Neurobiol 158: 298-306,
Goodman M. Phylogenetic comparisons suggest that distance from 2007.
the locus control region guides developmental expression of primate 122. Llanos AJ, Riquelme RA, Sanhueza EM, Hanson MA, Blanco CE,
beta-type globin genes. Proc Natl Acad Sci U S A 103: 3186-3191, Parer JT, Herrera EA, Pulgar VM, Reyes RV, Cabello G, Giussani DA.
2006. The fetal llama versus the fetal sheep: Different strategies to withstand
96. Joy SD, O’Shaughnessy R, Schlabritz-Loutsevitch N, Leland MM, hypoxia. High Alt Med Biol 4: 193-202, 2003.
Frost P, Fan-Havard P. Fetal blood sampling in baboons (Papio spp.): 123. Llanos AJ, Riquelme RA, Sanhueza EM, Herrera E, Cabello G, Gius-
Important procedural aspects and literature review. J Med Primatol 38: sani DA, Parer JT. Regional brain blood flow and cerebral hemispheric
151-155, 2009. oxygen consumption during acute hypoxaemia in the llama fetus. J
97. Julian CG, Vargas E, Armaza JF, Wilson MJ, Niermeyer S, Moore LG. Physiol 538: 975-983, 2002.
High-altitude ancestry protects against hypoxia-associated reductions 124. Longo LD. Carbon monoxide in the pregnant mother and fetus and its
in fetal growth. Arch Dis Child Fetal Neonatal Ed 92: F372-F377, exchange across the placenta. Ann N Y Acad Sci 174: 312-341, 1970.
2007. 125. Longo LD. Respiratory gas exchange in the placenta. In: Farhi LE, Ten-
98. Julian CG, Wilson MJ, Lopez M, Yamashiro H, Tellez W, Rodriguez ney SM, editors. Handbook of Physiology. Section 3. The Respiratory
A, Bigham AW, Shriver MD, Rodriguez C, Vargas E, Moore LG. Aug- System. Volume 4. Gas Exchange. Bethesda: American Physiological
mented uterine artery blood flow and oxygen delivery protect Andeans Society, 1987, pp. 351-401.
from altitude-associated reductions in fetal growth. Am J Physiol Regul 126. Longo LD. The Rise of Fetal and Neonatal Physiology: Basic Science
Integr Comp Physiol 296: R1564-R1575, 2009. to Clinical Care. New York: Springer, 2013, pp. 1-533.
99. Kamitomo M, Longo LD, Gilbert RD. Right and left ventricular func- 127. Longo LD, Ching KS. Placental diffusing capacity for carbon monoxide
tion in fetal sheep exposed to long-term high-altitude hypoxemia. Am and oxygen in unanesthetized sheep. J Appl Physiol 43: 885-893, 1977.
J Physiol 262: H399-H405, 1992. 128. Longo LD, Dale PS, Gilbert RD. Uteroplacental O2 uptake: Continuous
100. Kashiwazaki H, Suzuki T, Takemoto T. Altitude and reproduction of measurements during uterine quiescence and contractions. Am J Physiol
the Japanese in Bolivia. Hum Biol 60: 833-845, 1988. 250: R1099-R1107, 1986.
101. Keyes LE, Armaza JF, Niermeyer S, Vargas E, Young DA, Moore LG. 129. Longo LD, Delivoria-Papadopoulos M, Forster RE. Placental CO2
Intrauterine growth restriction, preeclampsia, and intrauterine mortality transfer after fetal carbonic anhydrase inhibition. Am J Physiol 226:
at high altitude in Bolivia. Pediatr Res 54: 20-25, 2003. 703-710, 1974.
102. Khaw KS, Ngan Kee WD. Fetal effects of maternal supplementary 130. Longo LD, Hill EP, Power GG. Theoretical analysis of factors affecting
oxygen during Caesarean section. Curr Opin Anaesthesiol 17: 309- placental O2 transfer. Am J Physiol 222: 730-739, 1972.
313, 2004. 131. Longo LD, Power GG, Forster RE. Respiratory function of the placenta
103. Kingdom JC, Kaufmann P. Oxygen and placental villous development: as determined with carbon monoxide in sheep and dogs. J Clin Invest
Origins of fetal hypoxia. Placenta 18: 613-621, 1997. 46: 812-828, 1967.
104. Kirschbaum TH, Dilts PV, Jr, Assali NS. Placental oxygen transfer in 132. Longo LD, Power GG, Forster RE. Placental diffusing capacity for
pregnant ewes during hyperbaric oxygenation. Pediatr Res 3: 398-406, carbon monoxide at varying partial pressures of oxygen. J Appl Physiol
1969. 26: 360-370, 1969.
105. Kiserud T, Acharya G. The fetal circulation. Prenat Diagn 24: 1049- 133. Lorenzo FR, Huff C, Myllymaki M, Olenchock B, Swierczek S, Tashi
1059, 2004. T, Gordeuk V, Wuren T, Ri-Li G, McClain DA, Khan TM, Koul PA,
106. Kiserud T, Rasmussen S. Ultrasound assessment of the fetal foramen Guchhait P, Salama ME, Xing J, Semenza GL, Liberzon E, Wilson
ovale. Ultrasound Obstet Gynecol 17: 119-124, 2001. A, Simonson TS, Jorde LB, Kaelin WG, Jr, Koivunen P, Prchal JT. A
107. Kiserud T, Rasmussen S, Skulstad S. Blood flow and the degree of genetic mechanism for Tibetan high-altitude adaptation. Nat Genet 46:
shunting through the ductus venosus in the human fetus. Am J Obstet 951-956, 2014.
Gynecol 182: 147-153, 2000. 134. Love GD, Grosjean E, Stalvies C, Fike DA, Grotzinger JP, Bradley AS,
108. Kitchen H, Brett I. Embryonic and fetal hemoglobin in animals. Ann N Kelly AE, Bhatia M, Meredith W, Snape CE, Bowring SA, Condon DJ,
Y Acad Sci 241: 653-671, 1974. Summons RE. Fossil steroids record the appearance of Demospongiae
109. Konje JC, Howarth ES, Kaufmann P, Taylor DJ. Longitudinal quantifi- during the Cryogenian period. Nature 457: 718-721, 2009.
cation of uterine artery blood volume flow changes during gestation in 135. Maginniss LA, Olszowka AJ, Reeves RB. Oxygen equilibrium curve
pregnancies complicated by intrauterine growth restriction. BJOG 110: shape and allohemoglobin interaction in sheep whole blood. Am J
301-305, 2003. Physiol 250: R298-R305, 1986.
110. Krebs C, Longo LD, Leiser R. Term ovine placental vasculature: Com- 136. Makowski EL, Hertz RH, Meschia G. Effects of acute maternal hypoxia
parison of sea level and high altitude conditions by corrosion cast and and hyperoxia on the blood flow to the pregnant uterus. Am J Obstet
histomorphometry. Placenta 18: 43-51, 1997. Gynecol 115: 624-631, 1973.
111. Lang U, Baker RS, Khoury J, Clark KE. Effects of chronic reduction 137. Makowski EL, Meschia G, Droegemueller W, Battaglia FC. Distribu-
in uterine blood flow on fetal and placental growth in the sheep. Am J tion of uterine blood flow in the pregnant sheep. Am J Obstet Gynecol
Physiol Regul Integr Comp Physiol 279: R53-R59, 2000. 101: 409-412, 1968.
112. Lang U, Baker RS, Khoury J, Clark KE. Fetal umbilical vascular 138. Martin DS, Khosravi M, Grocott MP, Mythen MG. Concepts in hypoxia
response to chronic reductions in uteroplacental blood flow in late-term reborn. Crit Care 14: 315, 2010.
sheep. Am J Obstet Gynecol 187: 178-186, 2002. 139. Mayhew TM, Jackson MR, Haas JD. Oxygen diffusive conductances
113. Lewis RM, Cleal JK, Hanson MA. Review: Placenta, evolution and of human placentae from term pregnancies at low and high altitudes.
lifelong health. Placenta 33 (Suppl): S28-S32, 2012. Placenta 11: 493-503, 1990.
114. Lichty JA, Ting RY, Bruns PD, Dyar E. Studies of babies born at high 140. McCullough RE, Reeves JT. Fetal growth retardation and increased
altitudes. I. Relation of altitude to birth weight. AMA J Dis Child 93: infant mortality at high altitide. Arch Environ Health 32: 36-39, 1977.
666-669, 1957. 141. Meschia G, Battaglia FC, Hay WW, Sparks JW. Utilization of substrates
115. Lindenburg IT, van Kamp IL, Oepkes D. Intrauterine blood transfusion: by the ovine placenta in vivo. Fed Proc 39: 245-249, 1980.
Current indications and associated risks. Fetal Diagn Ther 2014. 142. Meschia G, Cotter JR, Breathnach CS, Barron DH. The hemoglobin,
116. Lindow SW, Mantel GD, Anthony J, Coetzee EJ. A double-blind ran- oxygen, carbon dioxide and hydrogen ion concentrations in the umbili-
domised controlled trial of continuous oxygen therapy for compromised cal blood of sheep and goats as sampled via indwelling plastic catheters.
fetuses. BJOG 109: 509-513, 2002. 1965. Am J Obstet Gynecol 194: 1196, 2006.
117. Lingrel JB, Townes TM, Shapiro SG, Wernke SM, Liberator PA, Menon 143. Meschia G, Prystowsky H, Hellegers A, Huckabee W, Metcalfe J,
AG. Structural organization of the alpha and beta globin loci of the goat. Barron DH. Observations on the oxygen supply to the fetal llama. Q J
Prog Clin Biol Res 191: 67-79, 1985. Exp Physiol Cogn Med Sci 45: 284-291, 1960.
Volume 5, July 2015 1401
Placental Gas Exchange Comprehensive Physiology
144. Metcalfe J, Bartels H, Moll W. Gas exchange in the pregnant uterus. 172. Paulick RP, Meyers RL, Rudolph AM. Effect of maternal oxygen
Physiol Rev 47: 782-838, 1967. administration on fetal oxygenation during graded reduction of umbil-
145. Metcalfe J, Meschia G, Hellegers A, Prystowsky H, Huckabee W, ical or uterine blood flow in fetal sheep. Am J Obstet Gynecol 167:
Barron DH. Observations on the placental exchange of the respiratory 233-239, 1992.
gases in pregnant ewes at high altitude. Q J Exp Physiol Cogn Med Sci 173. Paulone ME, Edelstone DI, Shedd A. Effects of maternal anemia on
47: 74-92, 1962. uteroplacental and fetal oxidative metabolism in sheep. Am J Obstet
146. Mielke G, Benda N. Cardiac output and central distribution of blood Gynecol 156: 230-236, 1987.
flow in the human fetus. Circulation 103: 1662-1668, 2001. 174. Peeters LL, Sheldon RE, Jones MD, Jr, Makowski EL, Meschia G.
147. Miglino MA, Carter AM, Ambrosio CE, Bonatelli M, de Oliveira MF, Blood flow to fetal organs as a function of arterial oxygen content. Am
Dos Santos Ferraz RH, Rodrigues RF, Santos TC. Vascular organi- J Obstet Gynecol 135: 637-646, 1979.
zation of the hystricomorph placenta: A comparative study in the 175. Pena JP, Tomimatsu T, Hatran DP, McGill LL, Longo LD. Cerebral
agouti, capybara, guinea pig, paca and rock cavy. Placenta 25: 438-448, blood flow and oxygenation in ovine fetus: Responses to superimposed
2004. hypoxia at both low and high altitude. J Physiol 578: 359-370, 2007.
148. Miller FC, Petrie RH, Arce JJ, Paul RH, Hon EH. Hyperventilation 176. Penninga L, Longo LD. Ovine placentome morphology: Effect of high
during labor. Am J Obstet Gynecol 120: 489-495, 1974. altitude, long-term hypoxia. Placenta 19: 187-193, 1998.
149. Mills DB, Ward LM, Jones C, Sweeten B, Forth M, Treusch AH, 177. Piggott SE, Bogod DG, Rosen M, Rees GA, Harmer M. Isoflurane
Canfield DE. Oxygen requirements of the earliest animals. Proc Natl with either 100% oxygen or 50% nitrous oxide in oxygen for caesarean
Acad Sci U S A 111: 4168-4172, 2014. section. Br J Anaesth 65: 325-329, 1990.
150. Moore LG. Altitude, effects on humans. In: Encyclopedia of Reproduc- 178. Pijnenborg R, Vercruysse L, Hanssens M. The uterine spiral arteries
tion, Academic Press, 1999, pp. 107-112. in human pregnancy: Facts and controversies. Placenta 27: 939-958,
151. Moore LG. Comparative human ventilatory adaptation to high altitude. 2006.
Respir Physiol 121: 257-276, 2000. 179. Planavsky NJ, Reinhard CT, Wang X, Thomson D, McGoldrick P,
152. Moore LG, Brodeur P, Chumbe O, D’Brot J, Hofmeister S, Monge Rainbird RH, Johnson T, Fischer WW, Lyons TW. Earth history. Low
C. Maternal hypoxic ventilatory response, ventilation, and infant birth mid-Proterozoic atmospheric oxygen levels and the delayed rise of
weight at 4,300 m. J Appl Physiol (1985) 60: 1401-1406, 1986. animals. Science 346: 635-638, 2014.
153. Moore LG, Charles SM, Julian CG. Humans at high altitude: Hypoxia 180. Postigo L, Heredia G, Illsley NP, Torricos T, Dolan C, Echalar L, Tellez
and fetal growth. Respir Physiol Neurobiol 178: 181-190, 2011. W, Maldonado I, Brimacombe M, Balanza E, Vargas E, Zamudio S.
154. Moore LG, Jahnigen D, Rounds SS, Reeves JT, Grover RF. Mater- Where the O2 goes to: Preservation of human fetal oxygen delivery and
nal hyperventilation helps preserve arterial oxygenation during high- consumption at high altitude. J Physiol 587: 693-708, 2009.
altitude pregnancy. J Appl Physiol Respir Environ Exerc Physiol 52: 181. Power GG, Dale PS, Nelson PS. Distribution of maternal and fetal
690-694, 1982. blood flow within cotyledons of the sheep placenta. Am J Physiol 241:
155. Moore LG, Rounds SS, Jahnigen D, Grover RF, Reeves JT. Infant birth H486-H496, 1981.
weight is related to maternal arterial oxygenation at high altitude. J 182. Prychitko T, Johnson RM, Wildman DE, Gumucio D, Goodman M.
Appl Physiol Respir Environ Exerc Physiol 52: 695-699, 1982. The phylogenetic history of New World monkey beta globin reveals
156. Moore LG, Zamudio S, Zhuang J, Sun S, Droma T. Oxygen transport a platyrrhine beta to delta gene conversion in the atelid ancestry. Mol
in Tibetan women during pregnancy at 3,658 m. Am J Phys Anthropol Phylogenet Evol 35: 225-234, 2005.
114: 42-53, 2001. 183. Prystowsky H, Hellegers A, Meschia G, Metcalfe J, Huckabee W, Bar-
157. Moore WM, Battaglia FC, Hellegers AE. Whole blood oxygen affinities ron DH. The blood volume of fetuses carried by ewes at high altitude.
of women with various hemoglobinopathies. Am J Obstet Gynecol 97: Q J Exp Physiol Cogn Med Sci 45: 292-297, 1960.
63-66, 1967. 184. Reid DL, Parer JT, Williams K, Darr D, Phernetton TM, Rankin
158. Moraga F, Monge C, Riquelme R, Llanos AJ. Fetal and maternal JH. Effects of severe reduction in maternal placental blood flow on
blood oxygen affinity: A comparative study in llamas and sheep. Comp blood flow distribution in the sheep fetus. J Dev Physiol 15: 183-188,
Biochem Physiol A Physiol 115: 111-115, 1996. 1991.
159. Mortola JP, Frappell PB, Aguero L, Armstrong K. Birth weight and 185. Reshetnikova OS, Burton GJ, Milovanov AP. Effects of hypobaric
altitude: A study in Peruvian communities. J Pediatr 136: 324-329, hypoxia on the fetoplacental unit: The morphometric diffusing capacity
2000. of the villous membrane at high altitude. Am J Obstet Gynecol 171:
160. Mossman HW. The principal interchange vessels of the chorioallantoic 1560-1565, 1994.
placenta of mammals. In: DeHaan RL, Ursprung H, editors. Organo- 186. Rocco E, Bennett TR, Power GG. Placental diffusing capacity in
genesis. New York: Holt, Rinehart and Winston, 1965, pp. 771-786. unanesthetized rabbits. Am J Physiol 228: 465-469, 1975.
161. Mostello D, Chalk C, Khoury J, Mack CE, Siddiqi TA, Clark KE. 187. Rockwell LC, Keyes LE, Moore LG. Chronic hypoxia diminishes
Chronic anemia in pregnant ewes: Maternal and fetal effects. Am J pregnancy-associated DNA synthesis in guinea pig uteroplacental arter-
Physiol 261: R1075-R1083, 1991. ies. Placenta 21: 313-319, 2000.
162. Mott JC, Walker DW. Neural and endocrine regulation of circulation 188. Rudolph AM. Hepatic and ductus venosus blood flows during fetal life.
in the fetus and newborn. Comp Physiol 837-883, 2011. Hepatology 3: 254-258, 1983.
163. Mu J, Adamson SL. Developmental changes in hemodynamics of uter- 189. Rudolph AM, Heymann MA. Circulatory changes during growth in the
ine artery, utero- and umbilicoplacental, and vitelline circulations in fetal lamb. Circ Res 26: 289-299, 1970.
mouse throughout gestation. Am J Physiol Heart Circ Physiol 291: 190. Rurak DW, Richardson BS, Patrick JE, Carmichael L, Homan J. Blood
H1421-H1428, 2006. flow and oxygen delivery to fetal organs and tissues during sustained
164. Ngan Kee WD, Khaw KS, Ma KC, Wong AS, Lee BB. Randomized, hypoxemia. Am J Physiol 258: R1116-R1122, 1990.
double-blind comparison of different inspired oxygen fractions during 191. Rurak DW, Richardson BS, Patrick JE, Carmichael L, Homan J. Oxy-
general anaesthesia for Caesarean section. Br J Anaesth 89: 556-561, gen consumption in the fetal lamb during sustained hypoxemia with
2002. progressive acidemia. Am J Physiol 258: R1108-R1115, 1990.
165. Nicolaides KH, Campbell S, Bradley RJ, Bilardo CM, Soothill PW, 192. Soma H, Hata T, Oguro T, Fujita K, Kudo M, Vaidya U. Characteristics
Gibb D. Maternal oxygen therapy for intrauterine growth retardation. of histopathological and ultrastructural features of placental villi in
Lancet 1: 942-945, 1987. pregnant Nepalese women. Med Mol Morphol 38: 92-103, 2005.
166. Novy MJ, Frigoletto FD, Easterday CL, Umansky I, Nelson NM. 193. Soothill PW, Nicolaides KH, Rodeck CH, Bellingham AJ. The effect
Changes in umbilical-cord blood oxygen affinity after intrauterine trans- of replacing fetal hemoglobin with adult hemoglobin on blood gas
fusions for erythroblastosis. N Engl J Med 285: 589-595, 1971. and acid-base parameters in human fetuses. Am J Obstet Gynecol 158:
167. Owens JA, Falconer J, Robinson JS. Effect of restriction of placental 66-69, 1988.
growth on umbilical and uterine blood flows. Am J Physiol 250: R427- 194. Sorensen A, Peters D, Frund E, Lingman G, Christiansen O, Uldbjerg
R434, 1986. N. Changes in human placental oxygenation during maternal hyper-
168. Owens JA, Falconer J, Robinson JS. Effect of restriction of placental oxia estimated by blood oxygen level-dependent magnetic resonance
growth on oxygen delivery to and consumption by the pregnant uterus imaging (BOLD MRI). Ultrasound Obstet Gynecol 42: 310-314, 2013.
and fetus. J Dev Physiol 9: 137-150, 1987. 195. Sorensen A, Peters D, Simonsen C, Pedersen M, Stausbol-Gron B,
169. Palmer SK, Moore LG, Young D, Cregger B, Berman JC, Zamudio S. Christiansen OB, Lingman G, Uldbjerg N. Changes in human fetal
Altered blood pressure course during normal pregnancy and increased oxygenation during maternal hyperoxia as estimated by BOLD MRI.
preeclampsia at high altitude (3100 meters) in Colorado. Am J Obstet Prenat Diagn 33: 141-145, 2013.
Gynecol 180: 1161-1168, 1999. 196. Soria R, Julian CG, Vargas E, Moore LG, Giussani DA. Graduated
170. Parer JT. Reversed relationship of oxygen affinity in maternal and fetal effects of high-altitude hypoxia and highland ancestry on birth size.
blood. Am J Obstet Gynecol 108: 323-325, 1970. Pediatr Res 74: 633-638, 2013.
171. Parer JT. The effect of acute maternal hypoxia on fetal oxygenation and 197. Spotorno AE, Marin JC, Manriquez G, Valladares JP, Rico E, Rivas
the umbilical circulation in the sheep. Eur J Obstet Gynecol Reprod Biol C. Ancient and modern steps during the domestication of guinea pigs
10: 125-136, 1980. (Cavia porcellus L.). J Zool 270: 57-62, 2006.
1402 Volume 5, July 2015
Comprehensive Physiology Placental Gas Exchange
198. Stevenson GN, Collins SL, Welsh AW, Impey LW, Noble JA. A tech- 213. Wattel F, Mathieu D, Mathieu-Nolf M. A 25-year study (1983-2008) of
nique for the estimation of fractional moving blood volume by using children’s health outcomes after hyperbaric oxygen therapy for carbon
three-dimensional power doppler US. Radiology 132363, 2014. monoxide poisoning in utero. Bulletin de l’Académie Nationale de
199. Tchirikov M, Schlabritz-Loutsevitch N, Nathanielsz PW, Beindorff N, Médecine 197: 677-694, 2013.
Schroder HJ. Ductus venosus shunting in marmoset and baboon fetuses. 214. Weber RE, Kleinschmidt T, Braunitzer G. Embryonic pig hemoglobins
Ultrasound Obstet Gynecol 26: 252-257, 2005. Gower I (zeta 2 epsilon 2), Gower II (alpha 2 epsilon 2), Heide I (zeta
200. Tenenbaum DG, Piasecki GJ, Oh W, Rosenkrantz TS, Jackson BT. 2 theta 2) and Heide II (alpha 2 theta 2): Oxygen-binding functions
Fetal polycythemia and hyperviscosity: Effect on umbilical blood flow related to structure and embryonic oxygen supply. Respir Physiol 69:
and fetal oxygen consumption. Am J Obstet Gynecol 147: 48-51, 1983. 347-357, 1987.
201. Teng CC, Tjoa S, Fennessey PV, Wilkening RB, Battaglia FC. Transpla- 215. White MM, McCullough RE, Dyckes R, Robertson AD, Moore LG.
cental carbohydrate and sugar alcohol concentrations and their uptakes Effects of pregnancy and chronic hypoxia on contractile responsive-
in ovine pregnancy. Exp Biol Med (Maywood) 227: 189-195, 2002. ness to alpha1-adrenergic stimulation. J Appl Physiol 85: 2322-2329,
202. Teramo KA, Widness JA. Increased fetal plasma and amniotic fluid 1998.
erythropoietin concentrations: Markers of intrauterine hypoxia. Neona- 216. White MM, McCullough RE, Dyckes R, Robertson AD, Moore LG.
tology 95: 105-116, 2009. Chronic hypoxia, pregnancy, and endothelium-mediated relaxation in
203. Thaler I, Manor D, Itskovitz J, Rottem S, Levit N, Timor-Tritsch I, guinea pig uterine and thoracic arteries. Am J Physiol Heart Circ Physiol
Brandes JM. Changes in uterine blood flow during human pregnancy. 278: H2069-H2075, 2000.
Am J Obstet Gynecol 162: 121-125, 1990. 217. Wilkening RB, Meschia G. Fetal oxygen uptake, oxygenation, and
204. Thompson JA, Richardson BS, Gagnon R, Regnault TR. Chronic acid-base balance as a function of uterine blood flow. Am J Physiol
intrauterine hypoxia interferes with aortic development in the late ges- 244: H749-H755, 1983.
tation ovine fetus. J Physiol 589: 3319-3332, 2011. 218. Wilkening RB, Meschia G. Current topic: Comparative physiology of
205. Thorn SR, Rozance PJ, Brown LD, Hay WW, Jr. The intrauterine placental oxygen transport. Placenta 13: 1-15, 1992.
growth restriction phenotype: Fetal adaptations and potential implica- 219. Wilkening RB, Molina RD, Meschia G. Placental oxygen transport in
tions for later life insulin resistance and diabetes. Semin Reprod Med sheep with different hemoglobin types. Am J Physiol 254: R585-R589,
29: 225-236, 2011. 1988.
206. Thornburg KL, Louey S. Uteroplacental circulation and fetal vascular 220. Young M. Classics revisited: Researches on pre-natal life by Sir Joseph
function and development. Curr Vasc Pharmacol 11: 748-757, 2013. Barcroft. Placenta 13: 607-612, 1992.
207. Tissot van Patot MC, Murray AJ, Beckey V, Cindrova-Davies T, Johns 221. Yung HW, Hemberger M, Watson ED, Senner CE, Jones CP, Kauf-
J, Zwerdlinger L, Jauniaux E, Burton GJ, Serkova NJ. Human pla- man RJ, Charnock-Jones DS, Burton GJ. Endoplasmic reticulum stress
cental metabolic adaptation to chronic hypoxia, high altitude: Hypoxic disrupts placental morphogenesis: Implications for human intrauterine
preconditioning. Am J Physiol Regul Integr Comp Physiol 298: R166- growth restriction. J Pathol 228:554-564, 2012.
R172, 2010. 222. Zamudio S, Palmer SK, Droma T, Stamm E, Coffin C, Moore LG. Effect
208. Tissot van PM, Grilli A, Chapman P, Broad E, Tyson W, Heller DS, of altitude on uterine artery blood flow during normal pregnancy. J Appl
Zwerdlinger L, Zamudio S. Remodelling of uteroplacental arteries is Physiol 79: 7-14, 1995.
decreased in high altitude placentae. Placenta 24: 326-335, 2003. 223. Zamudio S, Postigo L, Illsley NP, Rodriguez C, Heredia G, Brima-
209. Tomimatsu T, Kakigano A, Mimura K, Kanayama T, Koyama S, Fujita combe M, Echalar L, Torricos T, Tellez W, Maldonado I, Balanza E,
S, Taniguchi Y, Kanagawa T, Kimura T. Maternal hyperventilation Alvarez T, Ameller J, Vargas E. Maternal oxygen delivery is not related
during labor revisited: Its effects on fetal oxygenation. Reprod Sci 19: to altitude- and ancestry-associated differences in human fetal growth.
1169-1174, 2012. J Physiol 582: 883-895, 2007.
210. Van Hoesen KB, Camporesi EM, Moon RE, Hage ML, Piantadosi CA. 224. Zamudio S, Torricos T, Fik E, Oyala M, Echalar L, Pullockaran J,
Should hyperbaric oxygen be used to treat the pregnant patient for acute Tutino E, Martin B, Belliappa S, Balanza E, Illsley NP. Hypoglycemia
carbon monoxide poisoning? A case report and literature review. JAMA and the origin of hypoxia-induced reduction in human fetal growth.
261: 1039-1043, 1989. PLoS One 5: e8551, 2010.
211. van Kamp IL, Klumper FJ, Bakkum RS, Oepkes D, Meerman RH, 225. Zhu R, Huang X, Hu XQ, Xiao D, Zhang L. Gestational hypoxia
Scherjon SA, Kanhai HH. The severity of immune fetal hydrops is increases reactive oxygen species and inhibits steroid hormone-
predictive of fetal outcome after intrauterine treatment. Am J Obstet mediated upregulation of Ca(2+)-activated K(+) channel function in
Gynecol 185: 668-673, 2001. uterine arteries. Hypertension 64: 415-422, 2014.
212. Watson AL, Skepper JN, Jauniaux E, Burton GJ. Susceptibility 226. Zhu R, Xiao D, Zhang L. Potassium channels and uterine vascular
of human placental syncytiotrophoblastic mitochondria to oxygen- adaptation to pregnancy and chronic hypoxia. Curr Vasc Pharmacol
mediated damage in relation to gestational age. J Clin Endocrinol Metab 11: 737-747, 2013.
83: 1697-1705, 1998.
Volume 5, July 2015 1403
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Mrcog Part 2-550 MCQS, Emqs and SaqsDocument529 pagesMrcog Part 2-550 MCQS, Emqs and SaqsSai Khin Aung Tint75% (4)
- Teratogenicity and Teratogenic Factors: AbbreviationsDocument5 pagesTeratogenicity and Teratogenic Factors: AbbreviationsItzel HernadezNo ratings yet
- Dechan IniDocument57 pagesDechan IniandikabrainNo ratings yet
- Albofera ThePhilippines'BabyFactorDocument2 pagesAlbofera ThePhilippines'BabyFactorALBOFERA, PRAISE GEE L.No ratings yet
- Vet Obst Lecture 8 Uterine Torsion in Domestic AnimalsDocument19 pagesVet Obst Lecture 8 Uterine Torsion in Domestic AnimalsgnpobsNo ratings yet
- MiscarriageDocument1 pageMiscarriageJen BallesterosNo ratings yet
- Tretinoin Cream: For Topical Use Only Acne TreatmentDocument2 pagesTretinoin Cream: For Topical Use Only Acne TreatmentredscrubsinNo ratings yet
- 2 PLACENTA PREVIA Case PresentationDocument19 pages2 PLACENTA PREVIA Case PresentationAiswarya ThomasNo ratings yet
- KEMH Full RecommendationsDocument18 pagesKEMH Full RecommendationsHo ManNo ratings yet
- Handbook For RMNCH CounsellorsDocument82 pagesHandbook For RMNCH CounsellorsJennifer Pearson-Paredes100% (1)
- 06 Reducing Perinatal & Neonatal MortalityDocument68 pages06 Reducing Perinatal & Neonatal MortalityrositaNo ratings yet
- Multiple Pregnancy: Kevin AndrewDocument36 pagesMultiple Pregnancy: Kevin AndrewintanpurnNo ratings yet
- Maternal ExamsDocument37 pagesMaternal ExamsMarianne Baquilala100% (2)
- Maternity QuestionsDocument49 pagesMaternity Questionsdeb100% (17)
- Action Error Ethos Political Ontology AsDocument333 pagesAction Error Ethos Political Ontology AsNayeli Gutiérrez HernándezNo ratings yet
- Ielts 200 ESSAYSDocument105 pagesIelts 200 ESSAYSIqbal SinghNo ratings yet
- The Dynamics of Team: An Interactive Workshop On Facilitating Effective Teams in Perinatal SettingsDocument23 pagesThe Dynamics of Team: An Interactive Workshop On Facilitating Effective Teams in Perinatal SettingskcochranNo ratings yet
- ThesisDocument11 pagesThesispriyankaNo ratings yet
- Chapter 27 ViolenceDocument28 pagesChapter 27 ViolenceSraddha PatelNo ratings yet
- Diabetes Mellitus by DR RelliqueteDocument5 pagesDiabetes Mellitus by DR RelliqueteKenneth Jed M. RobentaNo ratings yet
- Reflections (Prelims)Document6 pagesReflections (Prelims)Jasha MaeNo ratings yet
- Assignment Course Title: Measurement & Evaluation in Education Course Code: Pde 5109 MATRIC NO: PDE/19/0136 Name: Morakinyo, Olayemi ADocument15 pagesAssignment Course Title: Measurement & Evaluation in Education Course Code: Pde 5109 MATRIC NO: PDE/19/0136 Name: Morakinyo, Olayemi Aolayemi morakinyoNo ratings yet
- Dara Brodsky MD, Mary Ann Ouellette MS APRN IBCLC-Primary Care of The Premature Infant (2007)Document312 pagesDara Brodsky MD, Mary Ann Ouellette MS APRN IBCLC-Primary Care of The Premature Infant (2007)Hisham Elkilaney100% (1)
- Random FactsDocument298 pagesRandom FactsglemeseNo ratings yet
- MCN 1Document5 pagesMCN 1Aijem RyanNo ratings yet
- Team-Based Care of Women With Cardiovascular Disease From Pre-Conception Through Pregnancy and PostpartumDocument15 pagesTeam-Based Care of Women With Cardiovascular Disease From Pre-Conception Through Pregnancy and PostpartumJesús MorenoNo ratings yet
- Respiratory Physiology & NeurobiologyDocument14 pagesRespiratory Physiology & NeurobiologyRaul DoctoNo ratings yet
- OBCDocument53 pagesOBCAZERGEZERNo ratings yet
- Fetal DistressDocument22 pagesFetal DistressFathimath0% (1)
- Mendoza Jose David B. Module 6Document5 pagesMendoza Jose David B. Module 6chlspat12No ratings yet