You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Change Management PlanDocument8 pagesChange Management Planmarilynwalcott84100% (1)
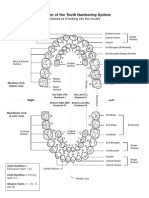
- Diagram of The Tooth Numbering SystemDocument1 pageDiagram of The Tooth Numbering Systemsaleh900No ratings yet
- Hope 3 Module 6 Quarter 2Document16 pagesHope 3 Module 6 Quarter 2Marchan Dalapo-Llacuna CorowanNo ratings yet
- Stream of NectarDocument4 pagesStream of NectarderekmendozaNo ratings yet
- Farmakoterapi Asma Dan COPD - 2Document32 pagesFarmakoterapi Asma Dan COPD - 2Camboy D' JablezNo ratings yet
- Case Study of DM Type 2Document1 pageCase Study of DM Type 2Camboy D' JablezNo ratings yet
- 2018 Management of Hepatitis BDocument13 pages2018 Management of Hepatitis BCamboy D' JablezNo ratings yet
- Global Burden of Cervical Cancer: A Literature Review: ArticleDocument10 pagesGlobal Burden of Cervical Cancer: A Literature Review: ArticleCamboy D' JablezNo ratings yet
- Asam - Basa: Sofia Fatmawati, M.Si., AptDocument16 pagesAsam - Basa: Sofia Fatmawati, M.Si., AptCamboy D' JablezNo ratings yet
- Perhitungan P4 AdeDocument17 pagesPerhitungan P4 AdeCamboy D' JablezNo ratings yet
- Baku PCT P4Document3 pagesBaku PCT P4Camboy D' JablezNo ratings yet
- Trucks DesigDocument116 pagesTrucks DesigEdgar Rojas EspejoNo ratings yet
- Molecular Etiopathogenesis of Ameloblastoma CurrentDocument5 pagesMolecular Etiopathogenesis of Ameloblastoma CurrentRiskha Febriani HapsariNo ratings yet
- The Influence of Temperature On The Operation of Batteries and Other Electrochemical Energy Storage SystemsDocument11 pagesThe Influence of Temperature On The Operation of Batteries and Other Electrochemical Energy Storage Systemssiraj udinNo ratings yet
- Basic Interior Design RulesDocument25 pagesBasic Interior Design RulesMadalina-Irina Tanaselea100% (2)
- b405 Manual SM - BvU3 2021Document886 pagesb405 Manual SM - BvU3 2021Andres PerezNo ratings yet
- SKF Masti PDFDocument108 pagesSKF Masti PDFmehrshad nedaeiNo ratings yet
- Edwards 7025 Barocel Gauge Instruction Manual - 2Document32 pagesEdwards 7025 Barocel Gauge Instruction Manual - 2dbhansali57No ratings yet
- 2004, Vol.22, Issues 2, The Clinical Use of Botulinum ToxinDocument90 pages2004, Vol.22, Issues 2, The Clinical Use of Botulinum ToxinRizweta Destin100% (1)
- Bolt Tightening Handbook Linear Motion ADocument44 pagesBolt Tightening Handbook Linear Motion AMarcos MorachickNo ratings yet
- SF9 CardDocument2 pagesSF9 CardJohn Marion CapunitanNo ratings yet
- Instructions For UseDocument16 pagesInstructions For UseMirkoNo ratings yet
- Subject: ACI-ICAO Implementing Annex 14 Course: (Cairo, Egypt, 28 June - 2 July 2020)Document2 pagesSubject: ACI-ICAO Implementing Annex 14 Course: (Cairo, Egypt, 28 June - 2 July 2020)Osama SharafNo ratings yet
- UntitledDocument16 pagesUntitledFelix YeboahNo ratings yet
- Physics 22 - The Nuclear AtomDocument13 pagesPhysics 22 - The Nuclear AtomMuhammad Amin SuhaimiNo ratings yet
- Harusdewi 2018Document7 pagesHarusdewi 2018Izzuddin AhmadNo ratings yet
- CHEMS Exchanger Edition 3Document16 pagesCHEMS Exchanger Edition 3Chems AdelaideNo ratings yet
- Beginners Guide CrossFitDocument5 pagesBeginners Guide CrossFitAdam 'Buddha' McGrath100% (2)
- MDR 9DDocument104 pagesMDR 9DDiana MarcelaNo ratings yet
- Practical Conduction of Department of Kriya ShariraDocument5 pagesPractical Conduction of Department of Kriya ShariraPranit PatilNo ratings yet
- Facilitative SupervisionDocument110 pagesFacilitative SupervisionPhilip Mutua100% (1)
- Elias Inorg Lec 4Document25 pagesElias Inorg Lec 4ashishNo ratings yet
- Periodicity of Metals - TeacherDocument6 pagesPeriodicity of Metals - TeacherTruong AnhNo ratings yet
- Grade 9 - Week - 4 - TLEDocument15 pagesGrade 9 - Week - 4 - TLEAlthea Marie MartinNo ratings yet
- Theories and Causes of Crimes: Chapter OneDocument29 pagesTheories and Causes of Crimes: Chapter OneJudessa Mae Pronce Cadacio100% (1)
- Electrophysiological Properties of Cardiac MyocytesDocument39 pagesElectrophysiological Properties of Cardiac Myocytesapi-19916399No ratings yet
- Babylog vn500 PDFDocument284 pagesBabylog vn500 PDFEdgar CarreraNo ratings yet