You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Plumbing PlansDocument4 pagesPlumbing PlansMarkNeilDeeNo ratings yet
- HSE-SAFETY-Plant Inspection ChecklistDocument3 pagesHSE-SAFETY-Plant Inspection ChecklistsantoshNo ratings yet
- The Newcastle-Ottawa Scale (NOS) For Assessing The Quality of Nonrandomized Studies in Meta-AnalysisDocument21 pagesThe Newcastle-Ottawa Scale (NOS) For Assessing The Quality of Nonrandomized Studies in Meta-Analysiscygnus112No ratings yet
- Gap Analysis - Sip 2019Document8 pagesGap Analysis - Sip 2019Brenda Cogasi100% (5)
- Knowledge Attitude and Barriers To The Use of Family Planning Among Married Men and Women at Fort Portal Hospital-Kabarole-Uganda.Document10 pagesKnowledge Attitude and Barriers To The Use of Family Planning Among Married Men and Women at Fort Portal Hospital-Kabarole-Uganda.KIU PUBLICATION AND EXTENSIONNo ratings yet
- Dar 03042019Document7 pagesDar 03042019Lawrence EmersonNo ratings yet
- Final MarkDocument32 pagesFinal MarkJhon Chiem OdtojanNo ratings yet
- Prescription AnalysisDocument16 pagesPrescription AnalysisMohd Azfar HafizNo ratings yet
- Behavior HomworkDocument5 pagesBehavior HomworkMariam AttounNo ratings yet
- Spring 02 LongDocument14 pagesSpring 02 Longbahrul.hidayah@yahoo.comNo ratings yet
- Naega-One Far Infrared Heat & Negative IonDocument6 pagesNaega-One Far Infrared Heat & Negative IonRoland MichaelNo ratings yet
- Electrical Appliances PDFDocument1 pageElectrical Appliances PDFcityofdarwingis0% (1)
- Revised Proposal Water TreatmentDocument13 pagesRevised Proposal Water TreatmentBryan Henson CarreonNo ratings yet
- Gizi Pranikah QR 2020Document28 pagesGizi Pranikah QR 2020rianNo ratings yet
- Saffola Cooking Oil Group F Sec EDocument9 pagesSaffola Cooking Oil Group F Sec EShiba Prasad MajhiNo ratings yet
- Arceo - Midterm Exam (Risk MGT)Document3 pagesArceo - Midterm Exam (Risk MGT)hello akotoNo ratings yet
- Release Form: A Manual For VolunteersDocument1 pageRelease Form: A Manual For VolunteersHuakailani School for GirlsNo ratings yet
- Principles of Fumigation (Basic) - CTSDocument48 pagesPrinciples of Fumigation (Basic) - CTSShyam Nayak100% (5)
- College of Teacher Education Second Semester, A.Y. 2020-2021 Population ProblemsDocument3 pagesCollege of Teacher Education Second Semester, A.Y. 2020-2021 Population ProblemsMIRANDA ALVINNo ratings yet
- Rational Psychotherapy and Individual PsychologyDocument9 pagesRational Psychotherapy and Individual PsychologyDavidNo ratings yet
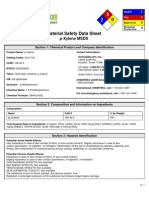
- XYLENE - MsdsDocument6 pagesXYLENE - MsdsNachiappan ViswanathanNo ratings yet
- The Importance of Nurse Caring BehaviorsDocument9 pagesThe Importance of Nurse Caring BehaviorsMelsa EchaNo ratings yet
- Coloring Book: Kid's Health & SafetyDocument16 pagesColoring Book: Kid's Health & SafetyGregoria ReyesNo ratings yet
- EPIDURALDocument3 pagesEPIDURALMarcos Jose WurschmidtNo ratings yet
- Activity Sheets in PHYSICAL EDUCATION 3rd QUARTERDocument6 pagesActivity Sheets in PHYSICAL EDUCATION 3rd QUARTERARLENE SEVILLENANo ratings yet
- Thurmolox PdsDocument3 pagesThurmolox PdsSinan A AzizNo ratings yet
- Denah ObatDocument2 pagesDenah ObatsafaridikaNo ratings yet
- Ulste June 2019Document246 pagesUlste June 2019SULINo ratings yet
- Todler InfoDocument2 pagesTodler Infoamedsegarra100% (1)
- Lecture 1 - Introduction To Secondary MetabolitesDocument36 pagesLecture 1 - Introduction To Secondary MetabolitesAlec LiuNo ratings yet