You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Resume 123Document3 pagesResume 123Jireh Alido FlavioNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Long Test 4th QuarterDocument4 pagesLong Test 4th QuarterJireh Alido FlavioNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Answer KeyDocument1 pageAnswer KeyJireh Alido FlavioNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Health Career SanielenDocument7 pagesHealth Career SanielenJireh Alido FlavioNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- SampleDocument8 pagesSampleJireh Alido FlavioNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Cheerdance 10Document15 pagesCheerdance 10Jireh Alido FlavioNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Title Page (Laz)Document1 pageTitle Page (Laz)Jireh Alido FlavioNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- CLP-Guide Full EDocument36 pagesCLP-Guide Full EVincent BautistaNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- ASEAN Strategic Plan For Culture and Arts 2016-2025Document3 pagesASEAN Strategic Plan For Culture and Arts 2016-2025Jireh Alido FlavioNo ratings yet
- GO 3 - 1 Evolution of Atomic TheoryDocument22 pagesGO 3 - 1 Evolution of Atomic TheoryJireh Alido FlavioNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Compost PitDocument3 pagesCompost PitJireh Alido FlavioNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
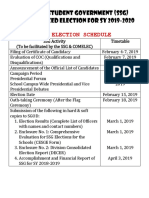
- SSG Election Schedule: Supreme Student Government (SSG) Synchronized Election For Sy 2019-2020Document1 pageSSG Election Schedule: Supreme Student Government (SSG) Synchronized Election For Sy 2019-2020Jireh Alido FlavioNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- PCOWord 01Document2 pagesPCOWord 01Jireh Alido FlavioNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Quiz Bee (2019)Document1 pageQuiz Bee (2019)Jireh Alido FlavioNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Class Prophecy 2019-2020Document6 pagesClass Prophecy 2019-2020Jireh Alido FlavioNo ratings yet
- Together With His Cousin, MR.: and The EloquentDocument3 pagesTogether With His Cousin, MR.: and The EloquentJireh Alido FlavioNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Buwan NG Kasaysayan: Contest Criteria Date & Time Venue Participants Materials JudgeDocument1 pageBuwan NG Kasaysayan: Contest Criteria Date & Time Venue Participants Materials JudgeJireh Alido FlavioNo ratings yet
- Functions of CommunicationDocument19 pagesFunctions of CommunicationJireh Alido FlavioNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Ipcrf Alibfinal 2nd Sem 2018Document10 pagesIpcrf Alibfinal 2nd Sem 2018Jireh Alido FlavioNo ratings yet
- Effective Speaking TechniquesDocument39 pagesEffective Speaking TechniquesJireh Alido FlavioNo ratings yet
- Functions of CommunicationDocument18 pagesFunctions of CommunicationJireh Alido FlavioNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Effective Speaking TechniquesDocument39 pagesEffective Speaking TechniquesJireh Alido FlavioNo ratings yet
- 05 21st Century Lit As v1.0Document14 pages05 21st Century Lit As v1.0Christian Paul Cortez Ditona100% (1)
- Network SecurityDocument159 pagesNetwork SecurityJireh Alido FlavioNo ratings yet
- Nursing Assessment of The Musculoskeletal SystemDocument14 pagesNursing Assessment of The Musculoskeletal SystemMargaret Philbin RobertsNo ratings yet
- Dynamic Warm-Up Exercises Instead of Traditional RoutinesDocument2 pagesDynamic Warm-Up Exercises Instead of Traditional RoutinespodamakriNo ratings yet
- O4p - Exercises - Posters Black WhiteDocument25 pagesO4p - Exercises - Posters Black WhiteFara AdhwaNo ratings yet
- What Are Isometric ExercisesDocument3 pagesWhat Are Isometric ExercisesHasan El TallissNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Workout 1: Chest and Back (Week 1)Document6 pagesWorkout 1: Chest and Back (Week 1)johnston_geoff438No ratings yet
- Post Stroke Functional Exercises For RehabilitationDocument37 pagesPost Stroke Functional Exercises For Rehabilitationjoel_simon_23100% (1)
- The Prevalence of Work-Related Musculoskeletal Disorders in Long-Distance Bus DriversDocument4 pagesThe Prevalence of Work-Related Musculoskeletal Disorders in Long-Distance Bus DriversSatria DananjayaNo ratings yet
- Bed PositionsDocument4 pagesBed PositionsJessa Kris RialubinNo ratings yet
- Sports Medicine Exam2020 QQ - 1Document22 pagesSports Medicine Exam2020 QQ - 1Volc100% (1)
- Kinesiology 1 Ospe Semester IDocument4 pagesKinesiology 1 Ospe Semester IEraj Khan100% (1)
- Muscle Mauler - Trigger Point Rolling EbookDocument27 pagesMuscle Mauler - Trigger Point Rolling EbookJanaka Wijeyesinghe100% (1)
- Dwipada Peetam: 8y S Ramaswami.. Trust6e, Krishnamacharya Yoga MandiramDocument6 pagesDwipada Peetam: 8y S Ramaswami.. Trust6e, Krishnamacharya Yoga MandiramPradosh Kumar PanigrahyNo ratings yet
- Rehabilitation of Rotator Cuff Tendinopathy: September 2014Document10 pagesRehabilitation of Rotator Cuff Tendinopathy: September 2014Adhitya TaslimNo ratings yet
- Achilles Repair ProtocolDocument19 pagesAchilles Repair ProtocolRobertNo ratings yet
- Push Oull Legs Training Master Class For CuttingDocument1 pagePush Oull Legs Training Master Class For CuttingShane WillyNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- SFS Assessment Guide PDFDocument12 pagesSFS Assessment Guide PDFJoao CunhaNo ratings yet
- 0701 Ergonomics Among GuitaristsDocument1 page0701 Ergonomics Among GuitaristssibieNo ratings yet
- Dance Injuries Power PointDocument20 pagesDance Injuries Power PointJerry Capitulo PorlucasNo ratings yet
- Pex 02 05Document5 pagesPex 02 05Tasha Magee100% (3)
- Calisthenics Mass - How To Maximize Muscle Growth Using Bodyweight-O.Document173 pagesCalisthenics Mass - How To Maximize Muscle Growth Using Bodyweight-O.hung35% (23)
- Hip Labral Repair PresentationDocument15 pagesHip Labral Repair Presentationapi-612728940No ratings yet
- Pex 02 01Document6 pagesPex 02 01Wijoyo KusumoNo ratings yet
- Aerial ManualDocument27 pagesAerial ManualValegria Alarcón100% (4)
- Elbow Orthosis: Prepared By: Jalil AhmadDocument11 pagesElbow Orthosis: Prepared By: Jalil AhmadJalil AhmadNo ratings yet
- P.E 101 Mod. 1 First Sem PDFDocument14 pagesP.E 101 Mod. 1 First Sem PDFabcdNo ratings yet
- Hip Flexor StrainDocument2 pagesHip Flexor StrainendurthiNo ratings yet
- The Front Lever Journey ?Document44 pagesThe Front Lever Journey ?Aldrei BaccayNo ratings yet
- Arthrogryposis Multiplex Congenita (AMC) in Siblings - Case Report. First DCMS Annual Research Day, April 7, 2018Document8 pagesArthrogryposis Multiplex Congenita (AMC) in Siblings - Case Report. First DCMS Annual Research Day, April 7, 2018Razi MohdNo ratings yet
- SLAP Tear Management in AthletesDocument11 pagesSLAP Tear Management in AthletesErnesto Dávila RamírezNo ratings yet
- Brachioradialis TestDocument1 pageBrachioradialis TestCatalina RzNo ratings yet
- Welcome to the Goddamn Ice Cube: Chasing Fear and Finding Home in the Great White NorthFrom EverandWelcome to the Goddamn Ice Cube: Chasing Fear and Finding Home in the Great White NorthRating: 4 out of 5 stars4/5 (59)
- Becky Lynch: The Man: Not Your Average Average GirlFrom EverandBecky Lynch: The Man: Not Your Average Average GirlRating: 4.5 out of 5 stars4.5/5 (15)
- Merle's Door: Lessons from a Freethinking DogFrom EverandMerle's Door: Lessons from a Freethinking DogRating: 4 out of 5 stars4/5 (326)
- Life Is Not an Accident: A Memoir of ReinventionFrom EverandLife Is Not an Accident: A Memoir of ReinventionRating: 3.5 out of 5 stars3.5/5 (7)
- Crazy for the Storm: A Memoir of SurvivalFrom EverandCrazy for the Storm: A Memoir of SurvivalRating: 3.5 out of 5 stars3.5/5 (217)