You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Leaders Eat Last Key PointsDocument8 pagesLeaders Eat Last Key Pointsfidoja100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
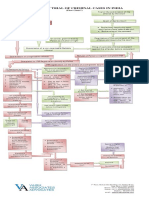
- Process of Trial of Criminal Cases in India (Flow Chart)Document1 pageProcess of Trial of Criminal Cases in India (Flow Chart)Arun Hiro100% (1)
- Mobile DevGuide 13 - Gulde For Mobile DeveloperDocument258 pagesMobile DevGuide 13 - Gulde For Mobile DevelopersmaliscribdNo ratings yet
- 39 Storey Treehouse Activity Pack PDFDocument11 pages39 Storey Treehouse Activity Pack PDFNeptune Shell0% (3)
- Piggery BookletDocument30 pagesPiggery BookletVeli Ngwenya100% (2)
- Ermita Malate Hotel Motel Operators V City Mayor DigestDocument1 pageErmita Malate Hotel Motel Operators V City Mayor Digestpnp bantay100% (2)
- PETITION For Declaration of NullityDocument7 pagesPETITION For Declaration of NullityKira Jorgio100% (3)
- The Wilderness - Chennai TimesDocument1 pageThe Wilderness - Chennai TimesNaveenNo ratings yet
- Material Safety Data Sheet Visco WelDocument4 pagesMaterial Safety Data Sheet Visco Welfs1640No ratings yet
- Ind Nifty ItDocument2 pagesInd Nifty ItRaghavendraNo ratings yet
- Book - India Physical EnvironmentDocument20 pagesBook - India Physical EnvironmentScience CoachingNo ratings yet
- Commercial Dispatch Eedition 6-13-19Document12 pagesCommercial Dispatch Eedition 6-13-19The Dispatch100% (1)
- Roy II vs. Herbosa, G.R. No. 207946, November 22, 2016Document20 pagesRoy II vs. Herbosa, G.R. No. 207946, November 22, 2016Rina OlandoNo ratings yet
- FAR MpsDocument2 pagesFAR MpsJENNIFER YBAÑEZNo ratings yet
- Xi'an City Sports Park Landscape Improvement ProjectDocument3 pagesXi'an City Sports Park Landscape Improvement ProjectGirija Sankar SahuNo ratings yet
- SAmple Format (Police Report)Document3 pagesSAmple Format (Police Report)Johnpatrick DejesusNo ratings yet
- Dragon Is The Fifth in The 12Document3 pagesDragon Is The Fifth in The 12Waylon CahiligNo ratings yet
- Whether To Use Their GPS To Find Their Way To The New Cool Teen HangoutDocument3 pagesWhether To Use Their GPS To Find Their Way To The New Cool Teen HangoutCarpovici Victor100% (1)
- Final Research Report - LP and AfDocument147 pagesFinal Research Report - LP and Afapi-636943816No ratings yet
- Pest Analysis PoliticalDocument4 pagesPest Analysis PoliticalAHMAD ALINo ratings yet
- Analytical ReasoningDocument7 pagesAnalytical ReasoningKashif NadeemNo ratings yet
- Way of St. LouiseDocument18 pagesWay of St. LouiseMaryann GuevaradcNo ratings yet
- Argumentative Essay-2Document4 pagesArgumentative Essay-2api-385385980No ratings yet
- MVP Teacher 12Document6 pagesMVP Teacher 12Ivan ChuNo ratings yet
- Tinniuts Today March 1990 Vol 15, No 1Document19 pagesTinniuts Today March 1990 Vol 15, No 1American Tinnitus AssociationNo ratings yet
- Welcome To UnixDocument14 pagesWelcome To UnixSrinivas KankanampatiNo ratings yet
- Feature Fusion Based On Convolutional Neural Netwo PDFDocument8 pagesFeature Fusion Based On Convolutional Neural Netwo PDFNguyễn Thành TânNo ratings yet
- Dolomite in Manila Bay A Big HitDocument3 pagesDolomite in Manila Bay A Big HitJoanaPauline FloresNo ratings yet
- 19.2 - China Limits European ContactsDocument17 pages19.2 - China Limits European ContactsEftichia KatopodiNo ratings yet
- CHC40221 Workplace LogbookDocument14 pagesCHC40221 Workplace LogbookKarla GiaNo ratings yet