You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Antidepressants (ME216) 20 5Document40 pagesAntidepressants (ME216) 20 5Dineish MurugaiahNo ratings yet
- How Selegiline (Deprenyl) Slows BrainDocument162 pagesHow Selegiline (Deprenyl) Slows Brainglaucoac9No ratings yet
- Pharma NotesDocument69 pagesPharma NotesJawad Ahmad100% (1)
- CYMBALTA (Duloxetine HCL) Product Monograph For CanadaDocument49 pagesCYMBALTA (Duloxetine HCL) Product Monograph For Canadajennabush100% (10)
- RitalinDocument6 pagesRitalinNavreetNo ratings yet
- Pharma Midterms Review UwuDocument11 pagesPharma Midterms Review UwuAJ BayNo ratings yet
- SSRI (Selective Serotonin Reuptake Inhibitor)Document1 pageSSRI (Selective Serotonin Reuptake Inhibitor)Mike EveretteNo ratings yet
- IyddDocument43 pagesIyddVikash KushwahaNo ratings yet
- Molecules 22 01192Document47 pagesMolecules 22 01192PuspaNo ratings yet
- AntidepressantsDocument33 pagesAntidepressantsAde Habibie100% (1)
- EULAR Revised Recommendations For The Management of FibromyalgiaDocument11 pagesEULAR Revised Recommendations For The Management of FibromyalgiaSUCIUNo ratings yet
- Elfspice's Compleat Acacia Extraction Guide: WarningDocument28 pagesElfspice's Compleat Acacia Extraction Guide: WarningDenys Konshyn100% (1)
- Major Depressive DisorderDocument11 pagesMajor Depressive DisorderJheanAlphonsineT.MeansNo ratings yet
- Chap 2Document20 pagesChap 2명수김No ratings yet
- Selective Serotonin Reuptake Inhibitors - Past, Present and Future - S. Stanford (Landes, 1999) WWDocument237 pagesSelective Serotonin Reuptake Inhibitors - Past, Present and Future - S. Stanford (Landes, 1999) WWKitty CristinaNo ratings yet
- Fluanxol Depot: Name of MedicineDocument11 pagesFluanxol Depot: Name of MedicineIvo_NichtNo ratings yet
- Pharmacology MnemonicsDocument91 pagesPharmacology MnemonicsKnizhonki Knizhonki96% (72)
- Neurobiology and Neuroprotective Benefits of Sleep.4 PDFDocument23 pagesNeurobiology and Neuroprotective Benefits of Sleep.4 PDFchanguito17No ratings yet
- PsychopharmacologyDocument77 pagesPsychopharmacologychachaazkaNo ratings yet
- K P Differential Diagnosis Pyramid: OPMAPS: Sychiatry EvisionDocument36 pagesK P Differential Diagnosis Pyramid: OPMAPS: Sychiatry EvisionArama CristiNo ratings yet
- Sample 100 MCQsDocument44 pagesSample 100 MCQsresearchphysio100% (3)
- Psychiatric Nursing Notes: Psych MedsDocument59 pagesPsychiatric Nursing Notes: Psych Medssurviving nursing schoolNo ratings yet
- Clomipramine PDFDocument18 pagesClomipramine PDFddandan_2No ratings yet
- Drugbank Ca-Amphetamine PDFDocument36 pagesDrugbank Ca-Amphetamine PDFIvo PalićNo ratings yet
- Clinical Pharmacokinetics of FluoxetineDocument14 pagesClinical Pharmacokinetics of FluoxetinePalwasha MalikNo ratings yet
- Treatment For Depression, FinalDocument12 pagesTreatment For Depression, FinalManya KrishnaNo ratings yet
- Depression Types, Causes, Symptoms, Risk Factor, and TreatmentDocument7 pagesDepression Types, Causes, Symptoms, Risk Factor, and TreatmentEditor IJTSRDNo ratings yet
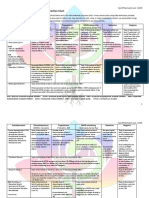
- Antidepressant & Psychedelic Drug Interaction ChartDocument3 pagesAntidepressant & Psychedelic Drug Interaction ChartFred The Nomad100% (2)
- Parkinson's Disease-Diagnosis & TreatmentDocument9 pagesParkinson's Disease-Diagnosis & Treatmentvivek_win95100% (1)
- Lesson Plan On Mental Health NursingDocument13 pagesLesson Plan On Mental Health NursingVarsha Rana100% (2)