You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Nutritional Management of SBS 2-18-17Document30 pagesThe Nutritional Management of SBS 2-18-17Julian MNo ratings yet
- Breastfeeding and Complementary FeedingDocument20 pagesBreastfeeding and Complementary FeedingJohn Christian LasalitaNo ratings yet
- Final Internship PresentationDocument25 pagesFinal Internship PresentationSaira JabeenNo ratings yet
- Nestle New Product Development Feb 06Document16 pagesNestle New Product Development Feb 06Raghav SagarNo ratings yet
- Infant Nutrition: of For Optimum andDocument35 pagesInfant Nutrition: of For Optimum andm mNo ratings yet
- Costco Vitamins USA 50Document3 pagesCostco Vitamins USA 50ankit3sharmaNo ratings yet
- Melc-Based Budget of Lessons in Mapeh - Health Grade 4 Quarter I Melc 1Document2 pagesMelc-Based Budget of Lessons in Mapeh - Health Grade 4 Quarter I Melc 1HECTOR RODRIGUEZ100% (4)
- Summative Test in Physical Education G-9 Test L. Multiple Choice: Select The Nearest Answer. Write Only The Letter of YourDocument4 pagesSummative Test in Physical Education G-9 Test L. Multiple Choice: Select The Nearest Answer. Write Only The Letter of YourArthur Capawing100% (1)
- RameyDocument15 pagesRameyPharmacist DinaNo ratings yet
- P.E and Health ReviewerrDocument14 pagesP.E and Health ReviewerrJoyce Anne Mae AdorioNo ratings yet
- FP Lesson 4 Week 4Document34 pagesFP Lesson 4 Week 4Hannah TorrillaNo ratings yet
- Chapter 7 Northern Mindanao and Davao RegionDocument8 pagesChapter 7 Northern Mindanao and Davao RegionGraceCayabyabNiduaza100% (1)
- Project-Proposal-Final-2 2Document5 pagesProject-Proposal-Final-2 2Kenneth Sarangaya100% (5)
- NSF284Document24 pagesNSF284yusrawasim147No ratings yet
- 40800-Article Text-177251-2-10-20220620 PDFDocument8 pages40800-Article Text-177251-2-10-20220620 PDFNur HamsyahNo ratings yet
- Epreuve 6eDocument2 pagesEpreuve 6emokouembefrancois2No ratings yet
- CPG DyslipidemiaDocument26 pagesCPG DyslipidemiaRenzy SalumbreNo ratings yet
- Guidelines For Nutritional Care of Preterm InfantsDocument7 pagesGuidelines For Nutritional Care of Preterm InfantsA. Berenice GarcíaNo ratings yet
- Chapter 41: Nursing Management: ObesityDocument2 pagesChapter 41: Nursing Management: ObesityPrince K. TaileyNo ratings yet
- Coco Palm Dhuni Kolhi All Inclusive Package 1920Document1 pageCoco Palm Dhuni Kolhi All Inclusive Package 1920TourListNo ratings yet
- Single Cell Proteins: As Nutritional Enhancer.: Adedayo, M.R . Ajiboye, E.A., Akintunde, J.K. Odaibo, A.Document11 pagesSingle Cell Proteins: As Nutritional Enhancer.: Adedayo, M.R . Ajiboye, E.A., Akintunde, J.K. Odaibo, A.Vj ReddyNo ratings yet
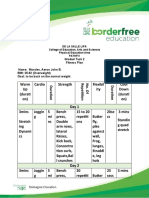
- Graded Task 2 - Fitness PlanDocument4 pagesGraded Task 2 - Fitness PlanMa Andrea TabiosNo ratings yet
- PizzaDocument10 pagesPizzaLenard TaberdoNo ratings yet
- Animals 10 01840 v2Document11 pagesAnimals 10 01840 v2Ging OcayNo ratings yet
- Paper J.sir - CbseDocument13 pagesPaper J.sir - CbseJabez JeenaNo ratings yet
- ELS16 Practicer Exam 5Document9 pagesELS16 Practicer Exam 5Kranting TangNo ratings yet
- Sweet PotatoDocument22 pagesSweet PotatoNegero ArarsoNo ratings yet
- Nutrition Reflection PaperDocument5 pagesNutrition Reflection Paperapi-312897235100% (1)
- Year8ScienceHomeLearning Cycle10Document7 pagesYear8ScienceHomeLearning Cycle10SheikhNo ratings yet
- Whole Brain Learning System Outcome-Based Education: Agri-Fishery Arts 11Document26 pagesWhole Brain Learning System Outcome-Based Education: Agri-Fishery Arts 11Mario Reynaldo CicatNo ratings yet